Page 1, 2, 3, 4
Early Animal and Cell Studies
Siegel (1979) observed increased cell detachment at low exposure. This relates to problematic embryo implantation and fetal growth restriction.15 The study was discussed in the WHO Criteria 22 as a reason to deny routine DUS.
Cachon (1981) observed damage to cell microtubules with only 10 seconds exposure16 at low intensity of 8mW/cm2.17 The study was discussed in the WHO Criteria 22 as a reason to deny routine DUS.
Ellisman (1987) observed myelination disruption at the extremely low intensity of 0.135mW/cm2.18 This is a rat pup study emulating the human fetal scenario. No serious discussion followed this essential, devastating study of DUS. Though initially given a high quality rating by the National Institutes of Health (NIH), it was later denied funding for continuation.19
Beverley Beech, of AIMSUK, characterizes the importance of animal studies:20
Over the years there have been numerous studies on rats, mice and monkeys which have found reduced fetal weight in babies... in the monkey studies, the ultrasound babies sat or lay around the bottom of the cage, whereas the little control monkeys were climbing up the bars and were up to the usual monkey tricks... What happens when the monkeys grow up?... as Jean Robinson has pointed out, monkeys do not learn to read, write, multiply, sing opera, or play the violin.20
1991: Intensities Increase by 8x
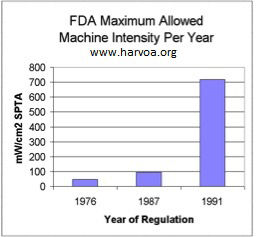
This great historical event marks the huge increase in DUS intensities and epidemics of childhood disease. During 1991, FDA negotiations among "interested parties" resulted in an 8x15x increase in allowable DUS machine intensities with safety responsibility entirely on the operator.21
 Since 1976, negotiations have always had a proposition on the table for unlimited machine intensities. This is to ensure that technological progress is not obstructed. D.L.Miller (2008) says: Since 1976, negotiations have always had a proposition on the table for unlimited machine intensities. This is to ensure that technological progress is not obstructed. D.L.Miller (2008) says:
[T]o liberalize the upper limit categories in some way to avoid inhibiting the [technological] development of diagnostic ultrasound and restricting the patient benefit which should follow [from the technological development]. 22
FDA provides some guidelines and special limits regarding intensity and exposure duration. However, the 720mW/cm2 limit applies for nearly all prenatal applications, even for the very sensitive eye of the fetus. This represents a dangerous paradox: The FDA intensity limit for the adult eye is 50mW/cm2. The limit for the fetal eye is 720mW/cm2. D.L. Miller says:
The new [DUS] limits were essentially made uniform across [application] categories, except for [adult] opthalmological examinations, for which consideration of possible heating indicated exceptional risk to the [adult] eye lens. The obstetrical ultrasound limit for the SPTA intensity was elevated to the highest 720 mW/cm2….22
The bracketed text is mine. The brackets shouldn't be necessary, i.e., D.L. Miller, if not under censure, should have been forthright enough to discuss this paradox, which is known to him but not his readership.
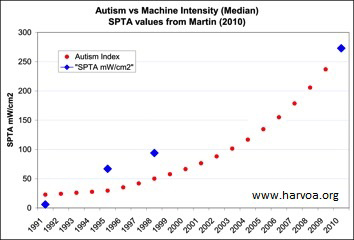
It should not be surprising that from 1991 onward, rising machine intensity levels23 correlate with rising autism incidence.24 See graph.
Inappropriate Science
As intensities and disease increased, did the NIH step up, appropriately fund studies? No. The opposite. Only a few studies were conducted after 1991. Most of these studies found ultrasound hazardous but were denied funding for continuance, and/or, their observations were ignored.
The IACC, a federal agency, directs U.S. tax dollars to autism research.25 Funds go almost entirely towards genetic studies, a few environmental studies, and no ultrasound studies.26 There resides industry's great profit and low liability.
From 1950 to the mid-1980s, there were over 700 studies reporting ultrasound-induced bioeffects, yet without resolution of human risk.27 Anderson and Barrett (1979) write:
The medical application of low-energy ultrasound as a diagnostic aid has developed in the absence of appropriate studies of its hazards.28
Ellisman (1987) says:
Several reviews of the literature… reveal that most studies were inadequately designed or inconclusive for the human medical situation; information on exposure conditions was frequently incomplete, markedly different from diagnostic ultrasound or in some instances sample size and follow-up were less than optimal.18
No Science
Worse than inappropriate science is no science. Abramowicz (2013) says:
…for fetal imaging, the ISPTA was allowed to increase by a factor of almost 16 from 1976 and almost 8 from 1986 to 1992, yet… all epidemiological information available regarding fetal effects predates 1992.29
D.L. Miller says:
[As of 1992] the allowable output for obstetrical ultrasound was increased [8x15x]… There has been little or no subsequent research… to systematically assess potential risks to the fetus….30
D.L. Miller is authoritative, funded by the NIH. With his humble admission of "little or no research," he confirms the dismal state of ultrasound science. With his silence, he denies the powerful existence of ultrasound science that indicts DUS.
 Science vs Policy Science vs Policy
See the following table, "Science vs Policy." The exposure ratios provide a stunning measure of the disjunct between science and public policy. I would have graphed this data, but the differences would be too large to be visualized unless the axes were compressed logarithmically.
The table contains three science studies (Siegel,15 Cachon,16 and Ellisman18) and two official policy statements (AIUM, FDA). The studies specify intensities where damage was observed. The policies specify intensities of official safety thresholds.
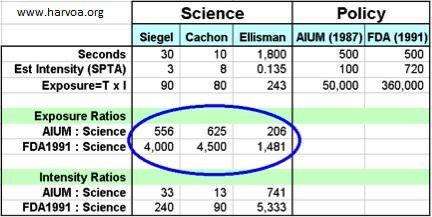
With exposure ratios, I compare science versus policy. Ratios are calculated by dividing policy exposures by science exposures. The ratios are huge, i.e., the difference between science and policy is huge.
The three studies above were selected for their low exposures. They have never been properly discounted by the mainstream. Example of impropriety: Del Cerro (1994) claims to have overturned Ellisman but did not use Ellisman's expert methods. It claims to have duplicated Ellisman, but it did not.31 Ellisman is a renowned neuroscientist. The senior author of Del Cerro (1994) is Morton W. Miller, a botanist, accused of incompetence and conflicts of interest with the radiation industries. For example, Andrew Marino, PhD, writes, "With reference to performing experiments, he [M.W. Miller] stated, 'I follow the golden rule - he who has the gold makes the rules.'"32
There is no critical discussion regarding Del Cerro or Ellisman. Del Cerro is cited only when implying that Ellisman is moot.33 Not wanting to be too harsh on M.W. Miller, the reader is invited to confirm these views.
The usual industrial defense against indicting studies is, "Who would ever expose a fetus to such long dwell times?" Answer: Cachon is only 10 seconds. Siegel is only 30 seconds. Ellisman is 30 minutes (1,800 seconds). However, when its extremely low intensity is extrapolated to the very high clinical intensities of present-day, probable damage could be indicated within a few seconds exposure.
The disjunct between public perception and scientific reality is described by Jacques Abramowicz, MD, a highly respected authority, prestigious member of AIUM,34 professor, and consultant to ultrasound machine manufacturers.
If asked, the vast majority of end users (and patients) will respond that ultrasound is not Xrays and is completely safe. In reality, there is a marked lack of knowledge on effects of ultrasound in tissues being examined (bioeffects) among the majority of these end-users.35
Profit adores "a marked lack of knowledge."
Page 1, 2, 3, 4 |




