|
Page 1, 2, 3
Introduction
Men and women have the same sex hormones, made from cholesterol by our ovaries or testicles and adrenal glands. The body assumes male and female forms depending on how much of which hormone we make. This net effect is determined by enzymes, which produce our hormones and subtly "fine-tune" the messages that they deliver. One such critical enzyme is 5alpha-reductase (5α-R): When its effects go awry, the consequences can be dramatic – altering the body via its sex hormones and the nervous system through its neurosteroids.
In this report, men whose testosterone replacement is inappropriately 5α-reduced are examined, as are their treatment options and outcomes. The normal physiology of sex hormones involved with these cases is discussed, as are the causes of the problems and their solutions. The new frontier of 5alpha-reduced neurosteroids is next considered and relevant clinical literature is cited. Finally, women's abnormal 5alpha-reduced neurosteroid production and its causal relation to premenstrual dysphoric disorder (PMDD),premenstrual syndrome (PMS), and dysmenorrhea is introduced, cases of which will be studied in the upcoming companion to thisarticle.
Men's Testosterone Replacement: Case 1
Case 1 is a 36-year-old former professional athlete with autoimmune hypothyroidism and combined-type hypogonadism: low free testosterone but midrange normal gonadotrophic LH and FSH. Despite testosterone replacement therapy (TRT) with the maximum recommended dose of transdermal testosterone gel, 1.62% (4 pumps = 81 mg topically q.d., of which 10% is absorbed), he still hadsymptoms, including hot flashes, reduced libido, and episodic anxiety.He perceived his muscle mass reduced, despite vigorous daily workouts at the gym. Worse still, vertical diplopia had recently begun and it resisted diagnosis by a neuro-ophthalmologist. Were these complaints due to thyroid or testosterone – or something not revealed by his MRI?
He saw Doc for a thyroid tune-up. Although his immune system interfered with the free T3 test by RIA, the new dialysis, LC/MS-MS (ED/MS) method – not an immunological assay – showed how to achieve his best dose. With his thyroid treatment adjusted, the sex hormone levels in November 2014 looked acceptable:
Table 1
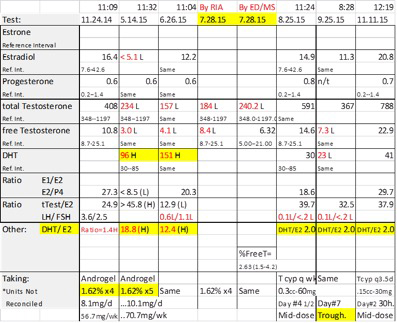
His diplopia and symptoms were greatly improved, but the man still felt subpar. Believing that he needed more testosterone, he increased his dose to 5 pumps, or 10.1 mg topical testosterone, daily – in excess of the manufacturer's recommended upper limit.1 After a brief improvement, he relapsed and within 6 months felt awful – as bad as he ever had! Even his puzzling vertical diplopia had fully relapsed. His repeated blood test results were revealing.
 The thyroid values looked fine, but his sex hormones were a bit of a shock: Estradiol (E2), total testosterone (tTEST), and free testosterone (fTEST) were all low. In contrast, his dihydrotestosterone (DHT) was high and the ratio of tTEST/DHT (comparing "total" with "total" measures) was only 2.4 – normally 9 to 12 (Table 1).2 Had the prescription hormone expired or been degraded? He got a fresh refill and repeated the tests: These results looked even worse. His LH and FSH were checked this time and were both low, too. Despite applying more testosterone, his sex hormone levels had fallen precipitously. Doc wondered, why? The thyroid values looked fine, but his sex hormones were a bit of a shock: Estradiol (E2), total testosterone (tTEST), and free testosterone (fTEST) were all low. In contrast, his dihydrotestosterone (DHT) was high and the ratio of tTEST/DHT (comparing "total" with "total" measures) was only 2.4 – normally 9 to 12 (Table 1).2 Had the prescription hormone expired or been degraded? He got a fresh refill and repeated the tests: These results looked even worse. His LH and FSH were checked this time and were both low, too. Despite applying more testosterone, his sex hormone levels had fallen precipitously. Doc wondered, why?
Contritely, Case 1 reduced his dose to 4 pumps but a month later felt no better, as confirmed by blood tests using ED/MS to rule out more immune interference. The tests consistently showed that his testosterone was being converted excessively to DHT. Doc found evidence that DHT can suppress the hypothalamus and thereby sex hormone production; apparently Case 1's high DHT had blocked his LH and FSH.3-5 Again, why?
A clue suggested the answer: His shoulders, to which he habitually applied the gel, had become excessively hairy. The factor responsible for this unpleasant turn of events is the enzyme 5α-R. A brief review of physiology is indicated.
Testosterone: Basic Sex Hormone Physiology
Surfing the web might lead one to believe that testosterone is the omnipotent conveyor of all things manly. It is not. Although androgenic (from the Greek, "creates men"), testosterone is best described as a prehormone. It offers itself on the altar of Differentiation to be converted either to estradiol and feminize women (via the enzyme aromatase, CYP19A1) – or conversely, by 5α-R to DHT, to the most powerfully masculinizing hormone.6
Compared with testosterone, DHT is about 10 times more potent at the androgen receptor (AR) in affecting its role to activate DNA transcription: DHT "fits" better to the AR, so it both stays bound longer and stimulates the receptor more strongly.7-10 This gives a biological benefit: In contrast with the two known estrogen receptors, there is but a single AR – the activity of adjacent 5α-R (or its lack) is an important means by which our body "diversifies" androgen signaling.9
In the developing fetus, sex hormones have important roles. In the male child, "weak" testosterone directs the development of most male internal sex organs, while the more potent DHT produces the external genitalia and prostate gland. The fetal brain is affected by sex hormone surges at circumscribed stages, and abnormalities of their timing or intensity are reported to influence children's subsequent development and behavior.11-16 Production of DHT is generally curtailed between the toddler years and puberty. Then, our bodies assume adult forms.
Converting testosterone to DHT provides a "one-way ticket to Macho City." Unlike testosterone, DHT cannot be aromatized to estrogens.17 However, we have seen that DHT is indeed able to feed back upon the hypothalamus (brain) to block the production of LH and FSH and thereby inhibit the production of all sex hormones.4,5 After DHT has served its function, it is eliminated – mostly by the liver (at which it arrives via blood, so blood tests are valid). Its breakdown products can have subtle effects, though not relevant to this discussion.
The Enzyme 5alpha-Reductase: Part 1
Enzymes are proteins (generally) made by the human body to hasten the conversion of a particular precursor (or substrate) into something different, a "product." Enzymes are coded in the DNA genome. By producing, activating, and degrading enzymes, the body controls its own structure, function and indeed, existence. The marvelous means by which all this is regulated evokes the Psalmist: we are fearfully and wonderfully wrought.
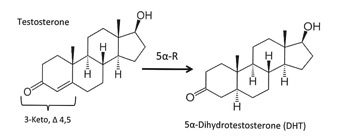
5 α-R was discovered in 1951. It cuts a double bond between the #4 and #5 carbon atoms in the A ring of its substrate steroids ("made from cholesterol") (Figure 1). Some of these are hormones – not just testosterone, but also progesterone, cortisol, and aldosterone. Others include hormone precursors (androstenedione, deoxy-corticosterone) and metabolites (epitestosterone).7
Figure 1
The significance of 5α-R began to be appreciated in 1968, when its deficiency in men was proved to cause the rare and extreme genetic condition male pseudohermaphroditism.18 We now understand that its importance is much greater.19,20
There are three variations (isoforms) of 5α-R (types 1–3), and two other proteins have similar effects. All five of these are shared by every eukaryotic organism – which can be quite primitive.7 This suggests that their importance is great. The importance for practitioners that these enzyme types respond differently to sundry pharmacological blockers will be discussed in Part 2 of this article.
These isoforms of 5α-R are expressed quite specifically in diverse tissues, and they vary with developmental age, to supply key locations with their products at the time that they are required. In the fetus, these tissues include the prostate, skin (genital development), and brain.7 The neonate widely expresses types 1 and 2, but after age 18 months, there is little 5α-R in the skin until puberty. Adult humans express 5α-R; men make far more than women.
The importance of an enzyme can be evaluated by studying animals – or humans – lacking it. Type 1 5α-R deficiency is not identified in nature, but engineered knockout mice have weak muscles and reduced bone mass.21 Type 2 deficiency gives men pseudohermaphroditism with ambiguous external genitalia and no prostate gland.18 Women, though, show few effects: reduced body hair, no acne, and high testosterone/DHT ratio.22 Humans without type 3 are severely retarded, with brain and eye defects indicative of a glycosylation disorder.23
Laboratory Tests for 5α-Reductase Activity
Commercially available laboratory tests can clinically indicate whether a person's 5α-R activity is appropriate for their sex: men have more, women have less. Blood tests are used to find the ratio of tTEST to total DHT. In healthy men, this tTEST/DHT ratio is said to fall between 9 and 12.2 From normal reference intervals and clinical observation, it may be argued that women's normal tTEST/DHT value is about 2.
 A second laboratory metric is the balance of 5alpha- to 5beta-reduced steroid metabolites (e.g., androsterone to etiocholanolone) in GC/mass-spec studies of 24-hour urine. Men have more 5alpha; women have more 5beta. This method has been employed in published research, and the tests are available to practitioners from several American reference laboratories, at least some of which routinely report a calculated 5α/ 5β balance.24-27 A second laboratory metric is the balance of 5alpha- to 5beta-reduced steroid metabolites (e.g., androsterone to etiocholanolone) in GC/mass-spec studies of 24-hour urine. Men have more 5alpha; women have more 5beta. This method has been employed in published research, and the tests are available to practitioners from several American reference laboratories, at least some of which routinely report a calculated 5α/ 5β balance.24-27
Case 1 Revisited
As hinted by his hairy shoulders, Case 1's skin is the probable source of the 5α-R that so thoroughly reduced his applied testosterone to DHT. Beginning shortly after conception, human skin produces 5alpha-reductase. Indeed, skin cells contain enzymes needed to produce every steroid hormone – and can contribute significantly to levels of circulating steroids.28
Clinicians: Case 1's problem is not unique. An early study of topical testosterone therapy found that although its use increased blood testosterone, patients' DHT gained relatively even more … and their tTEST/ DHT ratio decreased with transdermal TRT.2 The skin is implicated also in similar results from other studies: another of transdermal use and one of subcutaneous (pellet implant) TRT.29,30 The latter group reported high levels of DHT persisting for more than 100 days.
Case 1 had such dramatically abnormal blood tests because high DHT levels depressed his hypothalamic-pituitary LH and FSH production. This caused low testosterone, low estradiol, and the lack of their important effects. He felt bad because, yes, men also need the beneficial effects of some estrogen.31 Besides the milder androgenic effects of testosterone at the androgen receptor, its local conversion to estradiol has significant trophic effects on vascular endothelium, bone, and possibly other tissues.32-35
Elevated DHT can have other, less dramatic side effects which complicate men's testosterone replacement. These include erythro-cytosis, the over-production of red blood cells and vascular events from the consequently viscous, "sludgy" blood.36,37 There are complex relationships between testosterone, DHT, and prostate cancer as well, which also call attention to the role of proper sex hormone balance.38-40
Page 1, 2, 3
|




