|
Hair loss affects roughly 35 million men and 21 million women in the United States. Forty percent of men will have noticeable hair loss by age 35 and 65% of women will have noticeable hair loss by age 60. While hair loss mostly has cosmetic implications, there are many other conditions that manifest symptoms via hair loss. Hair loss definitely affects the life of its sufferers. The scalp and hairline play an important role in facial aesthetics. Receding hairline or hair loss imparts a loss of youth, health, and attractiveness, and results in a great degree of self-consciousness regarding the condition.
Possible causes of hair loss include sensitivity to dihydrotestosterone (DHT), a byproduct of testosterone; hormonal changes brought on as a result of medications, disease, and so on; injury to hair follicles as a result of chemotherapy; and trauma that alters hair growing and shedding phases.
Hair Loss Disorders
The most common hair loss disorder affecting men is male androgenetic alopecia. Male baldness is a genetically determined disorder characterized by the decrease in the size and activity of scalp hair follicles, as well as an atypical pattern of hair loss. Androgens (testosterone, dihydrotestosterone) are responsible for male pattern baldness. Testosterone is converted to dihydrotestosterone (DHT) by the enzyme 5-alpha-reductase. DHT acts on genetically susceptible hair follicles, causing their miniaturization, leading to hair follicle death. The gene can be inherited from the mother's or father's side. The onset, rate, and severity of hair loss are unpredictable. The disease severity increases with age and the condition is progressive. Male pattern baldness follows a pattern illustrated by the Norwood classification system.
Norwood Classification System
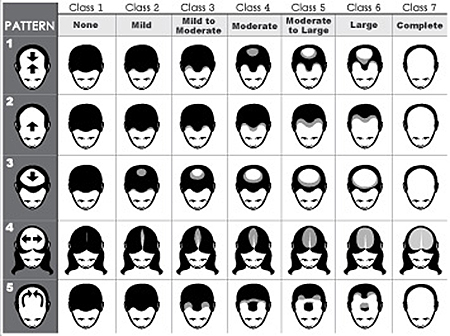
Female pattern hair loss is a common condition that refers to the decrease in central scalp hair density that occurs in females postpuberty. Female pattern hair loss affects more than 50% of women over age 50 and is emotionally devastating for its sufferers. Patterns of female androgenetic alopecia vary in appearance. Patterns that occur include diffuse hair thinning over the scalp, with more noticeable thinning toward the back of the scalp; diffuse hair thinning over the entire scalp, with more noticeable thinning toward the front of the scalp but not involving the frontal hairline; and diffuse hair thinning over the entire scalp, with more noticeable thinning toward the front of the scalp, involving and/or breaching the frontal hair line. Unlike male pattern hair loss, women experience miniaturization of hairs all over the affected areas of the scalp.
Treatment for Hair Loss
Hair loss can be addressed by a variety of treatment options. In this column, hormonal, pharmaceutical, herbal, laser and light devices, and surgical options will be discussed.
Hormonal Balancing
The hair follicle is an important site of hormone synthesis and metabolism. The hair follicle is able to regenerate new hairs as well as different types of hair via hormone regulation. As mentioned previously, the main hormones affecting hair follicles are the androgens. The androgens are capable of acting on the hair follicle in different ways – by stimulating hair growth, inhibiting hair growth, or causing no action.
Thyroid hormones (T3 and T4) have an effect on hair follicle functions such as cell turnover, pigmentation, and hair follicle cycling. Estrogens also alter hair follicle growth and its growth cycle by binding to estrogen receptors. Because of this, it is important that serum laboratory panels check hormone levels as part of the consultation for hair loss treatment.
Pharmacological Treatments
Currently, there are two medications that are FDA approved for androgenetic alopecia: minoxidil (Rogaine) and finasteride (Propecia). Minoxidil is a liquid that is applied to the scale where the hair loss occurs. Minoxidil was originally licensed as a drug to treat hypertension. Monoxidil slows the progression of hair loss and causes fine hair regrowth in 25% to 40% of males and 20% to 40% of females. The exact mechanism of action is unknown, but it is thought to work by improving circulation around the hair follicle or binding to the DHT receptors in the hair bulb. Rogaine is available over the counter and comes in 2% and 5% formulations.
Finasteride (Propecia) is a prescription medication that is FDA approved to treat male pattern hair loss. Propecia works by inhibiting the activity of the enzyme 5-alpha-reductase, which stops the conversion of testosterone into dihydrotestosterone (DHT). Finasteride has been shown clinically to reduce dihydrotestosterone levels in blood and in the scalp by up to 70%. DHT is the hormone responsible for the miniaturization of hair. Benefits of Propecia include slowing and/or cessation of hair loss and hair regrowth. Propecia cannot be used in females because it can produce feminization of genitalia in developing male fetuses. Finasteride and minoxidil are commonly used in combination for best results.
Nutraceuticals
There are a lot of nutraceuticals and botanicals on the market claiming to either promote hair growth or slow the hair loss process. Natural plant ingredients, vitamins, and minerals can be beneficial in hair conditioning, hair growth stimulation, and scalp dermatitis, as well as antiparasitic and antimicrobial agents. Nutraceuticals used as hair growth stimulants claim to promote hair growth via increased blood flow and circulation, increased nutrition, inhibition of DHT, and anti-inflammatory effects. Phytonutrients that may promote hair growth include ginkgo biloba, Chinese herb, ginseng, biotin, and marine proteins. Phytonutrients that may inhibit dihydrotestosterone (DHT) include saw palmetto, zinc, and vitamin B6. There is very little clinical research to substantiate the use of these nutrients, as they are not under the jurisdiction of the FDA, meaning that clinical trials proving their efficacy are not required.
Biotin is a vitamin commonly recommended for hair health. There is clinical evidence that biotin may benefit those suffering from alopecia areata. The theory of biotin as a hair supplement stems from the fact that biotin deficiency manifests as thinning of the hair and loss of hair color.
Another popular supplement for hair growth is Viviscal, an oral supplement composed of a proprietary mix of marine proteins, vitamin C, and horsetail extract. The ingredients are absorbed by the core of the hair follicle, strengthening the hair from the inside. Medical studies show that Viviscal use results in dramatic improvements in hair density, thickness, and length within 3 to 6 months.
Low Level Laser Light Therapy
A newer FDA-approved treatment modality for hair loss is low level laser light therapy. This treatment has been found to have a biomodulating effects on human hair and hair follicles. Clinical studies have shown that low level laser light provides cosmetic as well as physiologic benefits in hair restoration. Cosmetic benefits include increase in hair strength and overall improvement of hair fullness. Physiological benefits include the prevention of hair loss and stimulation of hair regrowth in areas of hair loss. It is suspected that the interaction of low level laser light therapy causes changes observed at the cellular level. The light is absorbed by the cells, stimulating energy production at the cellular level, improving cell function. The treatment is noninvasive and pain free, and can be performed in a medical office setting or with a home-use device. Results of low level laser light therapy include increased blood flow to the scalp, hair caliber, and hair density; improved hair texture and pigmentation; decreased hair shedding; and increased hair growth.
Surgical Options
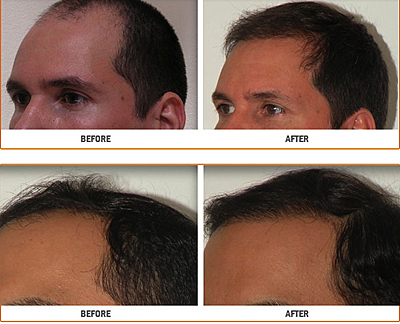
Hair transplantation surgery involves the repositioning of hair follicles from the rear of the scalp (donor area) to areas of thinning/balding (recipient area). Hair restoration surgery technique and equipment advances provide for a minimally invasive treatment with a natural hair appearance. There are two basic donor harvesting techniques: the strip level harvest technique and the follicular unit extraction technique. The strip harvest technique involves the removal of a horizontal strip of skin and hair follicles from the rear part of the scalp. The strip is dissected and transformed into individual grafts for reimplantation. In follicular unit extraction, individual follicular units (small groupings of one, two, or three hair follicles) are removed directly from the donor region using small punch incisions. The hair is then redistributed to the balding areas. Although follicular unit extraction is considered to be more time consuming and more dependent on the surgeon's skill, it does have many advantages, including a small, faster healing donor wound and less pain. Regardless of the method used, the transplanted hair retains its characteristics, color, texture, and growth rate after transplantation and regrowth. Following the procedure, small scabs may form in the graft sites. Usually, the hair grafts will shed in 2 to 4 weeks and new hair growth will begin in 3 to 4 months. Sometimes more than one session is necessary for optimum results.
Conclusion
Hair loss is a psychologically devastating condition for its sufferers. Androgenetic alopecia does not discriminate among sex, age, or ethnicity. Medicine has advanced to the point that many effective treatments are now available that can be used either alone or in combination to slow the process of hair loss. Patients should seek medical treatment for hair loss as soon as they notice hair shedding or hair thinning to diagnose and treat the problem. As with most medical conditions, early detection and prevention are key to successful outcomes.

References
Avram MR, Rogers NE. The use of low level laser light for hair growth: part I. J Cosmet Las Ther. 2009;11(2):110–117.
Camancho FM, Garcia-Hernandez MJ. Zinc aspartate, biotin, and clobetasol proprionate in the treatment of alopecia areata in childhood. Pediatr Dermatol. 1999 Jul–Aug;16(4):336–338.
Cassus A, Eskelinen A. A comparative study of a new food supplement, Viviscal® with fish extract for the treatment of hereditary androgenetic alopecia in young males. J Int Med Res. 1992;20:445–453.
Dua A, Dua K. Follicular unit extraction hair transplant. J Cutan Aesth Surg. 2010;3(2):76–81.
International Society of Hair Restoration Surgery. 2010 Hair Transplant Challenge Survey Results Summary.
Olsen EA, Dunlap FE, Funicella T, et al. A randomized clinical trial of 5% topical minoxidil versus 2% topical minoxidil and placebo in the treatment of androgenetic alopecia in men. J Am Acad Dermatol. 2002;47(3):377–385.
Rogers NE, Avram NR. Medical treatments for male and female pattern hair loss. J Am Acad Dermatol. 2008;59(4):547–566.
Rose PT. The latest innovations in hair transplantation. Facial Plast Surg. 2011;27(4):366–377.
Rossi A, Cantisani C, Scarno M, Trucchia A, Fortuna M, Calveri S. Finasteride, 1 mg daily administration on male androgenic alopecia in different age groups:10-year follow-up. Dermatol Ther. 2011;24(4):455–461.
Before and after surgery photos courtesy of Neograft Inc.
|



