Page 1, 2, 3, 4, 5
With rising challenges and diminished circulatory capacity, the physiologic strain on heart performance advances like falling dominos, inevitably resulting in degrees of kidney failure, deterioration of liver functions, accelerating diminution of gastric and pancreatic and hepatic secretions with progressive digestive impairments, peripheral circulatory embarrassment, and even organic brain syndrome. Obviously past lifestyle habits – tobacco and alcohol use, poor food choices, limited sleep, compromised stress adaptation patterns, licit and illicit drugs – create a setting (Claude Bernard's "internal milieu") in which all of these results from mitochondrial dysfunction can accelerate more rapidly than in others with more moderate health routines. Clearly the description offered can be observed over a matter of days or weeks in preterminal patients – or can be discerned by an astute practitioner some years (even decades) before the debilitations become obvious to others.
Putting Together the Bigger Map
While these ramblings might seem to have little to do with "cardiovascular diseases," ask yourself: "Should I be treating the damage from degenerative diseases while ignoring the environmental factors that persist and aggravate the condition?" That's rather like allowing the patient to wear the shoe causing the blister perhaps merely an hour or two a day. How foolish! Note that I do not ask whether the problem is with pipes, pump, or performance. The "diagnosis," in a classical sense, is almost irrelevant. The key is to establish the link between the condition and associated lifestyle choices and exposures so that a more comprehensive ([w]holistic!) approach can be used.
In effect, I am proposing that virtually all treatment for cardiovascular diseases should be aimed at the "utility" level. This example highlights this point: Whoever lives in a house, it matters not … the house has the "same" utilities as found with all other houses. Whether a baker, a banker, a teacher, a postman, you depend upon electricity coming in and light and heat going out, depend upon water coming in and drainage and sewage going out, depend upon food and supplies coming in and trash going out. Even a driveway coming in and roads going out!
Consider each "house" to be a single "cell" of the body. Thus, a neighborhood of similar houses would constitute an "organ" and a large cluster of assembled neighborhoods would comprise a "body." Our current medical paradigm aims at treating problems within specific neighborhoods. I propose that most of our treatments should be aimed at houses, at the utilities provided to and functioning within the individual cells. Regardless of which utilities or cells are suffering, those are the levels at which treatments should be aimed. This viewpoint encompasses a broader explanation of the symptoms and signs seen in illnesses, correlating the expression of disease in other organ systems (neighborhoods) that are likewise being affected by the impairment of their similar utilities.
Changing the Slope – Oh, No! Not Calculus!
As I propose this somewhat different approach to assessment and treatment, let me offer how I describe to patients our assessment and monitoring of their conditions. Our explanation induces patients to stay with treatment programs much longer than they did before. First, let me give homage to indices such as the SF-36 Health Survey.
Consisting of 36 items, the SF-36 is a brief survey designed to assess functional health and well-being in a variety of age, disease, and control populations. … Each question relates to one of eight domains: physical functioning, role-physical, bodily pain, general health perceptions, vitality, social functioning, role-emotional, and mental health. Results from these subscales contribute to scores for overall physical and mental health.3
In order to better address our particular patient population, I designed a customized "symptom-rating" form of about 50 items, printed on the flip side of our office visit notes page. At every doctor-patient visit, the patient rates his discomforts (from 0 to 10) before being seen. The various "positives" serve as foci for discussion at that meeting. Further, by "flipping up" the chart pages to earlier encounters, the progress of symptom reduction can be easily seen over time, from first visit to present time.
Graph:
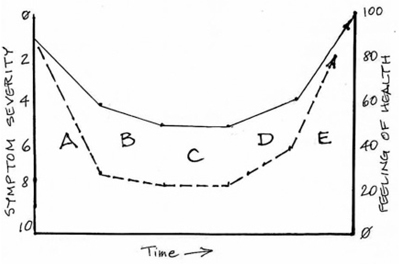
The demonstrative graph is easy for patients to understand. Assume that the patient has symptom complaints, rated on our 0-to-10 scale as shown on the left side. These roughly correlate inversely to the feeling of health and wellbeing, as shown from 0 to 100 on the right side. The patient presents with declining health and worsening symptoms, as noted by the solid line above the "A." During this first phase, your job is to define the underlying issues well enough to start improving the patient's condition … which means slowing the rate of worsening, as noted by the solid line above the "B." As you understand underlying causes better and work more with the patient, you work to hold most symptoms "level" or "unchanged," as noted by the solid line above the "C." This, in itself, is a major accomplishment … now you have the opportunity to make a real difference for this patient.
I describe to "newbie" patients that the first thing we're trying to do is to gain some understanding of what actually is affecting them. At this point, many patients usually will interrupt to share, once again, their various diagnoses (from other physicians), to be sure that I'm not overlooking their concerns. I acknowledge their statements and say that we understand that their various disease problems, as a whole, are worsening over time. They agree. I tell them that my first job is to identify the "pinch points," where doing something simple and deliberate will slow the rate at which they're worsening … then level them off, so that they're no longer worsening … then raise the slope of the curve, so that they're steadily improving … with the ultimate goal being to return them to more robust health, often better than that they've experienced in recent years.
This explanation encompasses a broader view of "health" more along the lines of Bircher, "a dynamic state of well-being characterized by a physical and mental potential, which satisfies the demands of life commensurate with age, culture, and personal responsibility."4
For those who need a more visual presentation, perhaps this graph might illustrate the concepts easier, since I do draw it "out in space" for patients:
During the next phase, as noted by the solid line above the "D," you are finally able to achieve some improvements and your patient clearly feels healthier. In the final phase, the solid line above the "E," results from your treatment patterns have become obvious and your patient is benefiting greatly. When you're able to establish a "maintenance program," your job is to monitor the hallmark symptoms carefully – along with relevant labs and exam findings – to "stay ahead of the curve," keeping most symptom severity scores at 3 or often less.
What about the dotted line on the graph? Some patients present to you as markedly more acute or chronically worse than anyone would like. "But doctor, I just found out about you. …" The steeper slope above the "A" shows that you have less time to evaluate and find successful treatments. Nevertheless, your job remains the same: slow the rate of worsening, find ways to hold everything "level" while you "buy time" for treatments to work (or to be identified), then work for gradual improvement and then much more aggressive changes.
Patients who are not themselves integrative medicine physicians can have only a brief, disjointed, and even mythical view of the roots of their problems, the diagnostic finesse often needed, and the treatment options available. What they clearly understand (or at least hope for) is that doing specific actions could lead to particular, desired results. Their motivation to continue their treatment programs comes only from successful responses. Since a patient has completed our same "SF-36-type" questions at each office visit, he or she can readily see the "march" of lower and lower "scores" away from "10" and toward "0" over the course of several office encounters.
Surprisingly, many improving patients quickly forget how bad they felt or how many limitations they suffered, so their own earlier scores are excellent reminders. In the end, when most of the answers are shifted left, "to the healthy side" (= 0 or just 1, maybe 2, occasionally 3), patients still have a visual reminder of where they started … and how much better and happier they now feel. And that is powerful motivation to continue the maintenance programs custom designed to retain their benefits gained. Repeatedly referring to this "graph" concept during the course of therapy can dramatically aid the patient to understand and comply with the testing and treatment programs, since they can visualize "where they are" in the plan of action.
Trowbridge's Idiot's Guidelines to Diagnosing Cardiovascular (and Other) Diseases
The following questions are essential:
1. Who is affected? Environmental exposures, other illnesses/operations?
2. What is the change (deviation) from normal structure/function?
3. When did these changes start? When have they progressed?
4. Where is the site of the ill organ/s? Of the patient (home/work/travel, present and past)?
5. Why did the change/s occur (preceding or associated events)?
6. How did the change/s develop and worsen? This is often the most critical question. …
The principal part of everything is the beginning. By answering these basic "reporter's questions," a good start can be made toward diagnosis and effective early treatment. Every patient starts here, no matter how complex or easy. Following this list reduces your likelihood of skipping an important factor and heading in the wrong direction. |
Trowbridge's '12-Step Program' of Don'ts and Do's*
Don't …
1. assume that the "other doctors" will appreciate your participation or any patient improvements;
2. assume that the condition has been correctly diagnosed or cannot be treated;
3. assume that the present medications are not contributing to or actually causing symptomatic complaints;
4. assume that a failing course is a likely outcome for this patient at this time;
5. assume that the treatments earlier prescribed by other doctors are correct or even required;
6. assume that nutritional support has little to contribute;
7. assume that any "diet" that has been earlier counseled is appropriate;
8. assume that oxygen saturation levels are sufficient, even when not grossly abnormal;
9. assume that an operation is the best next choice;
10. assume that activity level seen is the best that can be obtained;
11. assume that your patient understands anything at all about his/her condition, treatment, improvement, or worsening;
12. assume that your patient is at peace in his/her soul.
Do …
1. expect to educate your patient about the medical and political community as well as about costs and coverages for whatever you do – in person, through books and brochures, with your staff actively supporting;
2. expect that effective treatment can be started, literally, immediately and then improved upon;
3. expect that a substantial improvement is within easy reach;
4. expect that the rate of worsening can be slowed then halted for many patients … and then "better" is "within reach";
5. expect that your assessment will reveal alternatives that have been missed, disregarded, or ignored;
6. expect that proper supplements can be, in fact, life-saving;
7. expect that radical revision of food intake can be life-saving;
8. expect that supplemental oxygen can be life-saving;
9. expect that any patient can be better prepared to survive; any needed surgery … or to avoid it altogether;
10. expect that a gradual physical therapy program can be started immediately;
11. expect that you will need to explain the patient's condition (pipes/pump/performance, mito energy production, interrelated body functions, and so on) and basics of his/her treatment plans … often;
12. expect that crucial spiritual encounters can be lifesaving.
* These steps assume that appropriate medical treatment will be pursued concurrently, including detoxification of organic toxins or toxic heavy metals as needed.
Page 1, 2, 3, 4, 5 |




