Page 1, 2, 3
Supplementation
Nutritional supplementation has been effective with diabetes management. As mentioned above, various antioxidants are beneficial in preventing complications related to diabetes. The goal is to attempt to include as many fresh, nutrient-dense ingredients as possible and supplement as needed. High levels of oxidative stress have been found in diabetic patients, increasing the need for antioxidant supplementation. Deficient levels of vitamin C in diabetic patients are compounded by an impaired cellular uptake promoting hyperglycemia, which further decreases intracellular vitamin C levels. This localized deficiency contributes to end organ damage. Vitamin C supplements given at 1000 mg daily decreased urinary albumin and slowed the progression of diabetic nephropathy.4
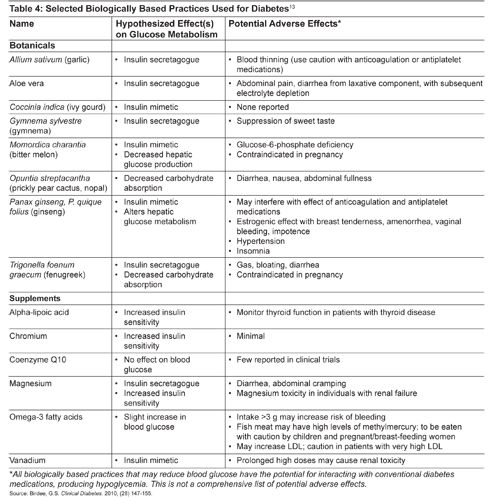
Electrolyte disorders have been found to play an important role in the complications of diabetes and are associated with increased mortality and morbidity. Several factors affect the body's ability to utilize nutrients, including nutritional status, absorption, acid-base imbalances, pharmacokinetics, renal disease, and acute illness. This might explain why diabetic patients are found to be low in several important nutrients. Hypomagnesemia is commonly identified in diabetic patients. Magnesium is involved with more than 300 enzymatic reactions and is vital to glucose metabolism and insulin homeostasis.14 Low serum and plasma levels of magnesium are associated with alterations in nerve, muscle, and cardiac conduction. This contributes to nephropathy and end stage renal disease. Nasri described a significant inverse relationship between serum magnesium and cholesterol levels.14 Liamis, Liberopoalos, Barkas, and Elisaf reported that an increased dietary intake of magnesium improved metabolic control and reduced the risk of T2DM and dyslipidemia.15
The trace element chromium aids glucose with transport into the cell. Chromium deficiency induces hyperglycemia and impaired glucose tolerance. Normal chromium intake is <20 ug/day. Diet recall was used to determine the daily dietary intake of chromium. Low daily intake led to supplementing with 200 ug chromium picolinate or chromium rich yeast, which resulted in improved glucose tolerance.4 The findings held true in cases of gestational diabetes mellitus.4 Chromium is found in whole grains, broccoli, and grapes. Normal dietary intake ranges from 20 to 35 ug/day, based on sex and age.9 Reduced HbA1C and fasting blood sugar levels were achieved with chromium supplementation. A large meta-analysis confirmed these results with a combination therapy of 600 ug chromium picolinide and 2 mg biotin.16
Biotin is a B vitamin that enhances chromium absorption and is involved with intracellular metabolism of glucose. Biotin administration of 9 to 16 mg/day improved glucose tolerance and decreased mean fasting blood sugar by 45%.4 Inositol, D-chiro-inositol, and D-pinitol are found naturally in legumes and citrus fruits. D-pinitol mediates the action of insulin. When given at 20 mg/kg of body weight, a 5% decrease in plasma glucose is seen.4 Vitamin D deficiency has been associated with increased glucose tolerance and diabetes. Supplementation has shown improvement in endothelial function and glucose tolerance, and an increase in insulin secretion. Doses varied from 800 to 300,000 IU/day.4
Alpha-lipoic acid (ALA) is an antioxidant. One of its many benefits includes preventing vitamin C and E deficiency, which are important to prevent and treat T2DM. Supplementing with 600 mg of ALA effectively increased insulin sensitivity, slowed the progression of complications, and prevented renal damage in T2DM patients. ALA is naturally occurring in broccoli, brussel sprouts, peas, potatoes, and yeast.17
Herbal Preparations
Bitter melon (Momordica charantia) is a plant native to India and Asia. It has been used medicinally for over 600 years. Evidence has shown positive effects on glucose levels, glucose uptake, glycogen synthesis, and glucose oxidation.17 Active ingredients include charantin, vicine, and polypeptide-p. Doses ranged from 150 and 2000 mg daily.18 Fruit, juice, and seed extracts were also used in some studies.16 Minimal side effects have been reported, although the ingredients are contraindicated in pregnancy.17 Four specific compounds identified provide the biological evidence for the benefits witnessed. An example of traditional or complementary medicine providing new and effective treatments for T2DM is metformin, which originated from goat's-rue (Galega officinalis). Tan and associates identified bitter melon as one of the most popular botanical treatments for T2DM.19
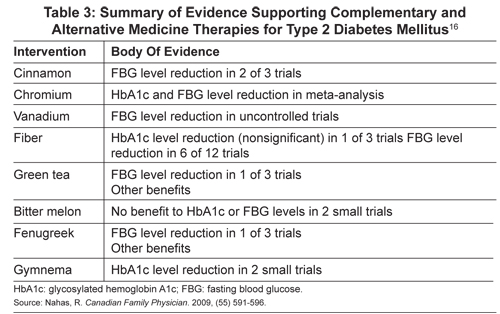
Another promising biologic T2DM treatment is fenugreek (Trigonella foenum-graecum). Commonly used in Traditional Chinese Medicine for glucose control, digestive aid, and relief of menopausal symptoms, fenugreek given at 100 mg improved fasting blood glucose levels.16 Fifteen grams of ground fenugreek seed power with a meal lowered postprandial glucose levels.17
Small trials have yielded promising results for Gymnema sylvestre, or gurmar. The leaves of this plant are used in Ayurvedic medicine to treat T2DM, high cholesterol, and obesity. Significant improvement in fasting blood sugar and HbA1C levels were obtained with doses from 200 mg to 800 mg of an extract daily.16
Cinnamon (Cinamonum cassia; gui zhi in Traditional Chinese Medicine) differs from the common spice Cinnamonum verum. C cassia has been used for thousands of years to treat T2DM. The herb activates insulin receptors and increases glycogen synthesis. Five clinical trials evaluated doses from 1 to 6 grams daily and saw decreases in fasting blood glucose levels from 18 to 29 %.16
Red Korean ginseng was found to improve glucose tolerance test results, fasting plasma glucose, and blood sugar levels.20 American ginseng (AG), along with an herb called konjac-mannan (KJM), may improve T2DM control and reduce complications. KJM affects the nutrient absorption rate in the small bowel, while AG affects the postabsorption activity; they work in unison to increase sensitivity and enhance secretion.21 Doses ranged from 100 to 200 mg twice a day. Reductions in fasting plasma glucose and HbA1C were documented.17
Berberine is a compound found in goldenseal, Oregon grape, barberry, and other plants. Research has shown it to be as effective as metformin. Doses up to 1000 mg twice daily along with lifestyle modifications led to a 7% reduction in HbA1C.22 Glucose- and lipid-lowering properties were identified. Future T2DM treatment may have been identified by targeting free fatty acid metabolism.23
Publication trends in Iranian endocrinology outlined articles effective in treating T2DM. Of the 44 articles found in PubMed, Scopas, and Google Scholar, a few of the relative topics include Silybum marianum L. Gaertn (silymarin, or milk thistle) as an effective treatment for T2DM. Decreased serum glucose and HbA1C levels were documented in diabetic outpatients using psyllium.24
Shenyan Kangfu, based on Traditional Chinese Medicine and Zhao Enjian's work, is a traditional herbal preparation that has been improved and formulated into tablets. These consist of 11 herbal ingredients with a synergistic effect to nourish the kidney and spleen by detoxifying the body. Widely acclaimed, Shenya Kangfu has been used for DM nephropathy, based on the qi-yin deficiency syndrome: swelling, fatigue, and weak limbs. Five sites in four major cities in mainland China have been identified. Enrollment is planned for 80 patients in stage III or IV diabetic nephropathy. Enrollment began in November 2012, and 20 participants had been enrolled by March 2013.25
As outlined, there are many alternative treatments for T2DM that have been recognized as safe and effective. Small trials, meta-analyses, and anecdotal evidence provide treatment recommendations and document safety concerns, while outlining the need for additional research to improve the care that clinicians provide. The Natural Medicine Comprehensive Database states that many treatments outlined in this article are safe and effective.17 The US Department of Health and Human Services contends that there is no high-quality evidence of benefit from alternative or supplemental treatments for diabetes.26 We as health-care providers must combine good judgment and available evidence to offer patients the best options for maintaining optimum health.
Chelation Therapy
Perhaps the most promising advance for the treatment of diabetes since insulin came from the Trial to Assess Chelation Therapy (TACT).27 This trial emerged from a hearing of the Oversight Committee of Congress and a subsequent call for proposals by the National Institutes of Health. TACT was designed to determine if future cardiac events could be reduced for patients at least 50 years of age who had already suffered at least one heart attack. It was a randomized, double-blind, clinical trial of 1708 patients, who were given more than 55,000 intravenous treatments. Half of the patients were given high-dose vitamins. Thus there were four groups in the study: double-placebo, high-dose vitamins without chelation, chelation with placebo vitamins, and chelation with high-dose vitamins.28 All of the patients were given evidence-based, conventional care for their coronary artery disease. At the beginning of the 5 years that patients were followed, they were given 30 weekly IVs and then 10 more treatments at monthly intervals.
The benefit of EDTA chelation was shown to be statistically significant. All of the cardiac events (death, reinfarction, stroke, coronary artery revascularization, and hospitalization for severe angina) were less in the EDTA groups than in the groups that received IV placebos. All-cause mortality was also less in the treated patients. Further analysis showed that 37% of the patients had diabetes (322 EDTA and 311 placebo). For those patients with diabetes, there was a 41% reduction in cardiac events, a 52% drop in recurrent MI, and a 43% reduction in deaths. Those who received both chelation and high-dose vitamins had the best results, but even with chelation and placebo vitamins, the NNT for major cardiac events for diabetic patients over the 5 years was 6.5. For statins in such patients, the NNT is considered to be highly effective at 17. Chelation was shown to be extremely safe when given according to protocol.27
A major action of EDTA chelation is its removal of toxic heavy metals, such as lead, cadmium, arsenic, and mercury. Such metals are proved toxic to the vascular tree from their free-radical activity.29 Carlos Lamar published numerous case studies in the mid-to-late 1960s on chelation's positive effects for diabetes.30 Paul Cutler found significant improvement in diabetic control with the use of the iron chelator, desferoxamine, in diabetic patients who also had high ferritin levels.31 EDTA also chelates iron, but not as effectively as desferoxamine. Therapeutic phlebotomies are more effective than either desferoxamine or EDTA. The vast majority of studies on chelation therapy and vascular disease were not randomized clinical trials and were of insufficient power to draw conclusions. Few studies identified patients who had diabetes.
The authors of TACT state that the magnitude of benefit for diabetic patients calls for urgency to replicate their study.32 TACT-2 has been planned to include only diabetic patients. At the same time, other forms of vascular disease, especially peripheral vascular disease, should be studied. Hancke and Flytlie published a remarkable study demonstrating that 24 out of 27 patients on the waiting list for amputation were able to cancel their surgery and save their legs.33 Chen Kuan-Hsing and associates demonstrated the effect of chelation therapy on progressive diabetic nephropathy in patients with T2DM and high lead levels.34
Page 1, 2, 3 |




