Page 1, 2, 3
What, then, can we accomplish with techniques such as this at our disposal? In order to organize the full range of clinical findings it is useful to have in mind the hierarchy of the brain's regulatory obligations. Considering the brain in its role as a control system, its principal burden is to assure its own unconditional stability. The method is very effective with brain instabilities such as migraines, panic attacks, asthma episodes, seizures, vertigo, night terrors, and even bipolar disorder. The training has been relatively ineffective to date for narcolepsy and sleep apnea, although it can be very helpful in isolated cases.
Remarkably, all of the above conditions respond well to a single protocol, which makes it plain that we are remediating a core vulnerability rather than specific conditions. The placement of choice is T3-T4 (in the international 10-20 system), which indicates that the functional deficit relates to the coordination between the two hemispheres. However, no claim of uniqueness is implied. The above conditions respond to a variety of other protocols as well. For example, a 90% favorable response for migraines was observed by Walker using QEEG-based methods.26 So the T3-T4 training is usually sufficient for the purpose, but it is not obligatory.
Remediating brain instabilities had been our strong suit from the moment that we first adopted the interhemispheric placement of T3-T4 in 1999. Up to that time we were using lateralized placements to target migraines that were typically also lateralized. When a particular migraine simply migrated to the other hemisphere when it was directly targeted, the interhemispheric placement was tried, and the migraine dissipated promptly. The interhemispheric placement soon became standard. It was the brain instabilities that mandated such a precise targeting in terms of frequency, and thus drove the agenda to ever lower frequencies.27
Next in the hierarchy is the issue of tonic state regulation, and within this broad category we have a hierarchy as well, one that conforms to our developmental sequence. Foundational in this hierarchy is the regulation of tonic arousal, which is in turn intimately connected with affect regulation, autonomic regulation, and interoception. This is the developmental priority in infancy and early childhood, and it is the primary target in ILF neurofeedback. Fortunately the deficits in these domains lie largely in the functional realm, quite irrespective of how intractable they may appear behaviorally. They are therefore accessible to us for remediation with neurofeedback.
Within the category of arousal regulation, we include insomnia, agitation, and hypervigilance, as well as general overarousal. Within the domain of affect regulation, we include the anxiety-depression spectrum, the capacity for attachment and empathy, and the personality disorders. Within the domain of autonomic regulation, we include dysautonomia, sympathetic/parasympathetic balance, regulation of blood pressure, heart rate, and vasoconstriction; peripheral temperature, galvanic skin response, and even gastric secretions (in connection with reflux). With respect to autonomic regulation, there is a substantial correspondence with traditional biofeedback utilizing measures of peripheral physiology.
Within the general category of state regulation we also encounter transient dyscontrol (quite possibly externally mediated) that is subsumed in the general category of behavioral disinhibition. It needs to be distinguished from brain instabilities. This category includes impulsivity, obsessive and/or compulsive behaviors, Tourette syndrome, bruxism, and rage behavior. Among these, Tourette syndrome and OCD present the greatest challenges to neurofeedback in its present state of maturity. Impulsivity, on the other hand, responds more consistently and is more completely resolved than the other conditions. In large group evaluations of ILF training for a general clinical population (5746 participants), the effect size was ~0.75 and the posttraining distribution in impulsivity was found to exceed the norm. These data have been presented in a professional forum, but have yet to be published. They are shown in Figure 1.
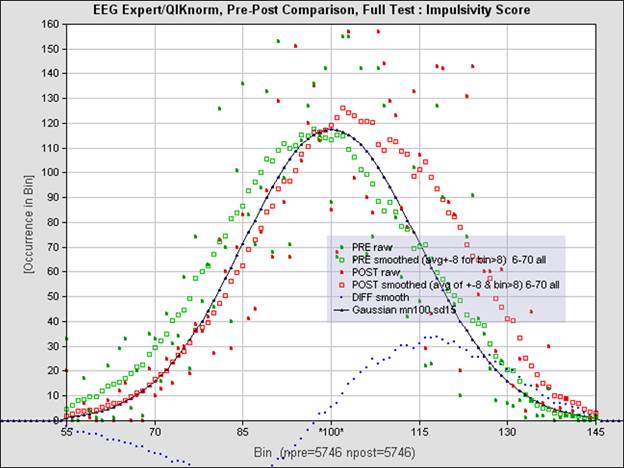
Figure 1: The plots show the distribution of impulsivity in terms of standard scores for a clinical population of 5746. The population is unselected, consisting of everyone in the customer base who had done the QIKtest both before and after 20 sessions of neurofeedback training. The training was offered for a variety of indications. The black curve shows the Gaussian distribution for the norming pool. The green curve illustrates the distribution prior to training; the red curve, posttraining. The data have been subjected to near-neighbor averaging for clarity. Improvement by nominally 0.75 standard deviations with training is indicated. The likelihood of scoring 2 standard deviations above the norm was doubled. The data are not naturally Gaussian-distributed. Nonparametric statistics were used throughout. Conversion from percentile scores to standard scores was performed for ease of interpretation.
The above observation illustrates that this kind of training is best regarded in the frame of training toward optimum brain function rather than as a technique to expunge dysfunction. The latter objective is accomplished by virtue of the former. That explains why the approach can rely on a modest number of electrode placements for all trainees. It is basic regulatory mechanisms common to us all that are being targeted in the training, not one or another specific deficit.
Beyond state regulation issues, we have the third category of regulatory burden; namely, responsiveness to the environment both on the input and on the output side. This category includes sensory processing issues, learning disabilities, maintenance of vigilance, attentional faculties, and working memory. It also includes motor planning and motor function such as speech articulation.
It was executive function that received most of the attention in neurofeedback in the early decades, mainly because this conformed to the interests of cognitive neuroscience. For the same reason, the training for the ADHD spectrum targeted the left hemisphere exclusively because that was the only one for which a cartography was available. The right hemisphere remained terra incognita; there was no point in even showing it in the textbooks (with the exception of the sensorimotor strip).
And yet clinical demands had driven us ever more toward lower frequencies and toward a right-hemisphere priority. Just as the left hemisphere has priority with respect to executive function, the right hemisphere has priority with respect to the foundational regulatory concerns of arousal, affect, and autonomic regulation. The right insula has a very different life experience from that of the left, so to speak. Since it was our most challenging clients that drove us ever lower in training frequency and ever more firmly onto the right hemisphere, it follows that the most intractable conditions encountered in mental health relate to vulnerabilities of right-hemisphere function first and foremost.28 Further, since we are driven to attend to the earliest developmental priorities of the developing infant, it follows that we are targeting the residual sequelae of early childhood trauma in much of our work.
Throughout the evolution of the training protocol schema over the last two decades, a remarkable consistency has been observed. The frequency at which right-hemisphere training optimizes for any individual differs systematically from that of the left. In the infralow frequency range, the left hemisphere training optimizes at twice the frequency of the right. In biological systems, it is the lowest frequency that sets the tone, and higher frequencies coordinate with the basic rhythm. A harmonic relationship is not unexpected. Within the conventional EEG frequency range, the right hemisphere optimizes at 2 Hz lower than the left. Here it is likely that the left hemisphere is taking the lead and the right hemisphere is the follower. The division of labor seems appropriate: The right hemisphere is in charge of our state of being, of our vegetative and our core or intrinsic self; the left hemisphere is in the lead when it comes to reacting to and engaging with the world. This view has recently received support from an evaluation of information flow within microstates.29
The implications for brain training are that we should understand the infralow frequency training principally in terms of right-hemisphere priorities, and we should understand training in the conventional EEG range in terms of left-hemisphere priorities. That is indeed how matters have unfolded over the years. The crossover between these two realms is at the only place that it can be; namely, at 2 Hz on the right hemisphere, which corresponds to 4 Hz on the left in both the high frequency and the low frequency perspectives. The frequency relationships are illustrated in Figure 2.
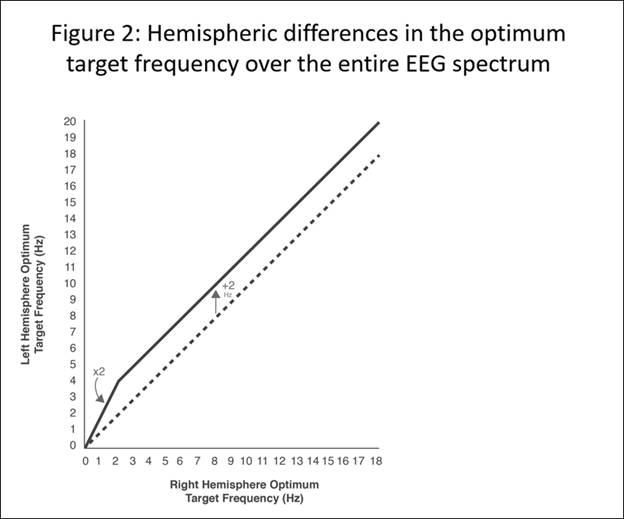
Figure 2: A fixed relationship prevails between the optimum response (target) frequencies in the left and right hemispheres. In the EEG range above 2 Hz, the left hemisphere training optimizes at 2 Hz higher than the right. Below 2 Hz, the relationship is harmonic. The left hemisphere training optimizes at twice the frequency of the right. This relationship holds throughout the infralow frequency region.
Fleshing out this model are frequency rules that relate interhemispheric training in the frontal and prefrontal region to training on the central strip, and those that relate the parietal and occipital interhemispheric training to that on the central strip. Collectively this model testifies to the specificity – as well as the subtlety – with which brain dynamics are organized on the large scale. It supports the presumption that the integrity of timing and frequency relationships are foundational to the harmonious functioning of the brain.
It should be observed in passing that the sole evidence for the above frequency rules consists of the collective subjective reports of trainees that allow the determination of the optimum training frequency in each case. No independent evidence for these frequency rules yet exists. There is not even any objective evidence for the existence of the optimum response frequency. So on the one hand, the findings fail to meet conventional research standards in terms of objective evidence, and on the other hand the posited relationships are likely among the most firmly established rules governing the dynamic organization of our neuronal networks. The frequency rules have been observed to hold consistently by thousands of clinicians who use them to guide their work. They hold over the entire range of frequencies that has been characterized, some four orders of magnitude.
The Current Status of Neurofeedback in Health Care
Collectively, we are still near the beginning of the journey of exploiting techniques such as neurofeedback for physical and mental health. But already much has been well established and the outlines of what is possible are becoming clear. All neurofeedback methods have their more specific and their more general effects, in that every brain challenge affects not only the specific mechanism being engaged but with it the whole brain as well. The particularity of the different methods means that no single one can be expected to satisfy all of the clinical objectives.
Among the principal approaches, infralow frequency training likely has the most comprehensive clinical footprint. The particular strength of the infralow frequency training is in application to the various trauma syndromes that afflict core state regulation, which must be the clinical priority.30 This includes in particular developmental trauma and the autism spectrum, where systematic remedies have clearly been lacking. It also includes the adult manifestations of early trauma such as dissociative identity disorder, borderline personality disorder, other personality disorders, and chronic pain syndromes. A case series for pediatric epilepsy utilizing ILF training has been published.31
Page 1, 2, 3 |




