

From the
Townsend Letter |
||
Recent Progress in Clinical Applications |
||
Continued. . . 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12
Fungi
Chart 4: Fungi Associated with Fibromyalgia and Other Pathologies
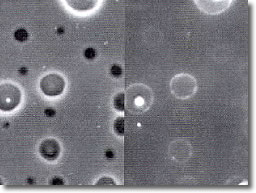
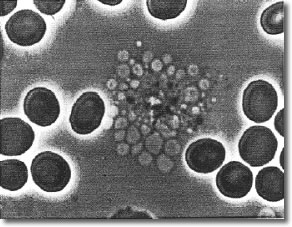
Life-threatening infections resulting from fungal pathogens such as Cryptococcus neoformans have been increasing steadily over the past ten years because of the prevalence of AIDS and the widespread use of immunosuppressive drugs.79 Mucormycosis is a devastating fungal disease affecting mainly diabetic and immunosuppressed patients and frequently causing death. Mucor rhizopus (black fungus), the opportunistic fungus, has been controlled by Sulfoxime™ and intravenous Amphotericin B. Most fungi have a strong antioxidant system and tolerate oxygen very well. The fungus Mucor has been associated with fibromyalgia55 and observed with the Bradford Peripheral Blood Assessments (BPBA). (See Photo 2, above.) Twenty systemic fungal infections arising within a five-year period were analyzed among cancer patients. Aspergillosis (black fungus) was the most common invasive fungal disease (55%), followed by mucormycosis (15%), and fusariosis (15%) from infection by Fusarium sp., a fungus which attacks almost all grains in the field, including wheat, corn, rice, and barley.121 (See Photo 2, above.) In this study 85% of the patients were diagnosed with black fungus utilizing the Bradford High Resolution Microscope; 100% of the FMS patients had black or red fungus. Melanin is a pigment widely dispersed in nature, found in hair, butterfly wings, beetles, the human brain (substantia nigra), black fungus, and many biological structures having a black appearance. Chemically, melanin is a three-dimensional polymer composed of several basic building blocks or monomers connected in a random manner. The precursor for many melanins is the amino acid phenylalanine, forming such substances as dopamine and L-dopa. C. neoformans is one example of several pathogenic fungi containing melanin granules, giving them a black appearance. Another example is Aspergillus niger or black bread mold.An examination of any of the melanins in an electron spin resonance (ESR) device reveals that melanin is a multi-site polymeric free radical containing stable unpaired electrons. This implies that melanin is capable of acting as a scavenger of free radicals (since free radicals annihilate each other) and is thereby able to protect a melanin-containing fungus from an oxidative burst released by immunocompetant cells.80 Additional studies have shown that there is indeed a transfer of electrons between melanin and free radicals present in the surrounding medium.81 These studies also demonstrate that some strains of melanin-containing fungus may differ in melanin content by as much as eightfold. Quantitative analysis revealed that melanin comprised greater than 15% of the dry mass of the cell after a ten-day growth in a medium supplying the necessary ingredients for melanin synthesis. The virulence of pathogenic strains of black fungi is shown to be directly related to the melanin content. Those fungi grown in media containing the precursors of melanin were more virulent than those deprived of these substances.82 A corollary to this research is that those suffering from infection by a melanin-containing (black) fungal pathogen should avoid foods that contain large amounts of phenylalanine. The food containing the largest amount of this amino acid is the soybean. Soybean products also include tofu and soymilk. Exposure of melanized black fungal cells to 0.1–0.5% sodium hypochlorite (NaOCl) bleached the cells white and abolished the ESR signal, consistent with melanin disruption.15 It may also be safely said that any substance tolerated by the body and supplying nascent oxygen would also be effective in bleaching melanin granules in vivo. A second example of such a substance is Proprietary Stabilized Active Oxygen Carrier, used in clinics worldwide for this purpose. C. neoformans is a human pathogenic fungus that is unusual in two respects: (1) it has a polysaccharide capsule similar to that found in encapsulated bacteria, and (2) it can produce melanin. Cells of C. neoformans are significantly more negatively charged than cells of baker's yeast (Saccharomyces cerevisiae). This negative charge is a repulsive force to the negative charge on circulating formed cells that conveys a degree of immunological privilege for most fungi. The polysaccharide capsule is responsible for the high negative surface charge. In addition, the melanin of this organism is also negatively charged, giving an increased negative charge per cell. It has been established that macrophage phagocytosis is affected by the electrical potential of targeted microorganisms.83 Cryptococcus neoformans must reduce ferric iron (Fe+3) to the ferrous form (Fe+2) before uptake. Detailed studies have shown that melanized cells reduce iron from the ferric to the ferrous state at a rate 16 times that of nonmelanized cells.84 Iron is required for the continued growth of this organism. If the melanin in melanized cells is bleached, the ability of this fungus to reduce iron to an available form is thereby thwarted. Intra-tracheal inoculation of C. neoformans strain 52 induced a vigorous T-cell-mediated pulmonary inflammatory response that controlled the growth of the organism. In contrast, strain 145 induced a pulmonary response that was delayed in onset, slower to develop, and ineffective in controlling the infection. These two strains differ only in melanin production with strain 52 low and strain 145 high. In addition, the high-melanin-containing strain 145 inhibited TNF-alpha production and lymphocyte proliferation by T-cells. By inhibiting the production of TNF-alpha by T-cells, melanin can inhibit the recognition of the organism by host defenses and block the resulting activation of apoptosis in this fungus.85 Various drugs are known to bind to melanin with high affinity, including the antipsychotic agent trifluoperazine and the antimalarial agent chloroquine. When C. neoformans was exposed to trifluoperazine, melanized cells were more susceptible than nonmelanized cells. Chloroquine had no fungicidal effect on either melanized or nonmelanized cells. These results suggest that antifungal drugs of the future intended to target melanized fungal cells may be found among those substances having a high binding affinity for melanin.86
|
||
![]()
Consult your doctor before using any of the treatments found within this site.
![]()
Subscriptions are available for Townsend Letter, the Examiner of Alternative Medicine magazine, which is published 10 times each year.
Search our pre-2001
archives for further information. Older issues of the printed magazine
are also indexed for your convenience.
1983-2001
indices ; recent indices
Once you find the magazines you'd like to order, please use our convenient form, e-mail subscriptions@townsendletter.com, or call 360.385.6021 (PST).

All rights reserved.
Web site by Sandy Hershelman Designs