Long Haulers
The COVID-19 pandemic has led to a huge uptick in folks moving from New York City. While some are remaining in suburbs and exurbs within the metropolitan area, not a few are doing big moves out of state. When I first heard the term “long hauler,” I immediately envisioned truckers who habituate the interstate freeways and take breaks at truck stops that are strange little worlds unto themselves; life at the truck stop ranges far beyond gassing up and greasy spoon dining, some of which typifies the illicit business seen at any busy port. It was a little bit of a surprise to discover that those individuals who have survived a bout with SARS-CoV-2 but remain symptomatic on a prolonged basis are calling themselves “long haulers,” evidently because they are dealing with the virus over the long haul; still I can’t get the big trucks out of my mind.
On the August 22 NPR Weekend Edition, a Texan epidemiologist described her own experiences as a COVID-19 long hauler.1 Many of the symptoms are not different from those that patients with chronic fatigue, fibromyalgia, chemical sensitivity, and Lyme disease experience: fatigue, exhaustion, muscle aching, muscle weakness, brain fog, lack of concentration, loss of endurance, depression, loss of sex drive, inability to carry out job duties and home chores, hypersensitivity, anxiety, hopelessness, and more. Dr. Margot Gage was not initially diagnosed with COVID-19 because she did not have a fever nor did she have a cough. She was healthy and physically fit before become symptomatic. Beyond the fatigue and brain fog, she experiences hot flashes that require keeping her home very cool, extreme sensitivity like an allergy when outside in the sun, loss of smell and taste, and any prolonged bout of work activity will result in exhaustion requiring bedrest. She connects with long haulers who experience other unusual symptoms, including weird skin rashes, visual difficulties, ringing in the ears, and nails growing very long while losing hair. Gage thinks that like other viral illnesses COVID-19 has a post-viral syndrome that relates to chronic fatigue syndrome.
Unfortunately, long haulers are being waitlisted to get care.2 While Mount Sinai Hospital in NYC opened its Center for Post-COVID Care in May, many hospitals and clinics across the country do not have such specialized centers. The online patient advocacy group, Survivor Corps, is seeking to change this absence urging for opening of many more specialty centers (survivorcorps.com). Long-haulers are no longer having symptoms of acute illness and presumably have negative rt-PCR tests so they are not contagious. But that does post a dilemma—when is the right time to treat a COVID-19 patient in the clinic setting to ensure staff and other patients are not exposed to the virus? A Yale University immunologist, Akiko Iwasaki, PhD, thinks that the long-hauler may still have active COVID-19 virus causing the prolonged symptoms. But Iwasaki also hypothesizes that “non-infectious virus in some cells trigger an immune response” responsible for chronic symptomatology.
If COVID-19 post-viral syndrome behaves similarly to other viral conditions, one would expect that IgM antibody testing would be negative, IgG testing would be positive, and other inflammatory and immune system markers would be abnormal. However, such testing has not yet been adequately defined.
RLC Labs Recalls Nature-Throid and WP Thyroid Hormone Products
On August 25, RLC Labs of Phoenix, Arizona, emailed a voluntary recall notice of its Nature-Throid and WP thyroid hormone products. The lab specified more than 20 individual lot numbers for 1/2, 1, and 2 grain products; it would appear that this list included all thyroid products sold by RLC during the past year. The recall notice “has been initiated because testing has found that the product may be sub-potent (i.e. less than 90% of the labeled amount of liothyronine or levothyroxine)…To date, there have been no reports of adverse events related to the recall.” Although this is a “voluntary” recall, RLC Labs specified to “immediately cease further distribution of the product and quarantine all quantities of unexpired product(s) within your possession. In addition, if you distributed product subject to this recall, please work to identify as soon as possible those customers to whom you delivered product(s) and notify them of this action.”

It is understandable when a drug company manufactures an adulterated product that a recall is necessary. What is not understandable is how all thyroid products manufactured by RLC Labs were “found to be sub-potent.” Does this mean that RLC Labs does not conduct quality control testing of individual lots to determine potency? It would make sense that a lot of thyroid hormone was not manufactured properly, but all lots were deemed questionable?
For the past decade there has been difficulty with thyroid hormone manufacturing, including proprietary Synthroid as well as Armour Thyroid. RLC Labs faced manufacturing difficulties a number of times resulting in no thyroid hormone availability. Why the lab was unable to manufacture thyroid hormone during these time periods has never been disclosed. In the past year RLC Labs managed to fulfill warehouse supplies in all potencies. Hence, it was quite shocking that the lab was obliged to recall its products now.
The putative reason for the recall was that inadequate thyroid hormone potency would result in failure to adequately treat thyroid deficiency based on the product’s listed strength. However, it is unclear what quality control measures were employed during the manufacturing process. Beyond thyroid hormone recall, integrative doctors should question the integrity of the unregulated vitamin/nutraceutical supplement industry. The possibility that a supplement does not contain the stated quantity of nutrients/herbs is very concerning. Professional grade supplement manufacturers claim to do routine quality control; products manufactured for direct consumer sale may not be doing quality control. However, as the thyroid recall process suggests, quality control testing may be sub-par. It would be appropriate for supplement manufacturers to be forthcoming on their quality control testing and agreeable to share such reports with health professionals.
Fibromyalgia
Our theme and cover story this issue focuses on fibromyalgia. As Leslie Axelrod, ND, discusses, fibromyalgia diagnosis is undiagnosed in more than 20% of patients while 10% of patients are mistakenly diagnosed with the condition. While physicians and patients think of fibromyalgia primarily as a condition of pain and weakness, symptomatically patients experience cognitive dysfunction, malaise, insomnia, orthostatic hypotension, hormonal imbalance, and susceptibility to infection. Axelrod notes that standard testing for inflammation such as Sed Rate and C-reactive protein are frequently normal. Recent research showed that studying cytokine activity of white blood cells following protein induction of cell division (mitogen activation) was dramatically reduced in fibromyalgia patients compared to normal controls. Fibromyalgia patients frequently demonstrate elevated IgG antibodies to viruses, including Parvo19, HHV-6, HHV-7, EBV, and enterovirus as well as bacteria, including H. pylori. Not infrequently, patients concurrently have parasites, mold mycotoxin, candidiasis, and Lyme disease.
Alan McDaniel, MD, frames fibromyalgia as the body’s inability to adapt to chronic stress. The hypothalamic-pituitary-adrenal axis (HPA-axis) upregulated by stress will initially overproduce cortisol but eventually depletes the adrenal reserve, leading to lower cortisol levels. Despite the fact that adrenal fatigue is a disputed diagnosis, reduced cortisol levels require nutrient and botanical support—if not cortisol replacement. Thyroid hormone testing generally limited to TSH frequently misses hypothyroidism. Although we generally think of insulin resistance’s role in diabetes and metabolic syndrome, McDaniel notes that it is essential to the stress response seen in fibromyalgia. IgG-mediated food allergies are more easily detected once hormone and metabolic dysfunctioning is addressed. McDaniel emphasizes that DHEA, cortisol, and pregnenolone may all need to be implemented to correct HPA-axis dysfunction.
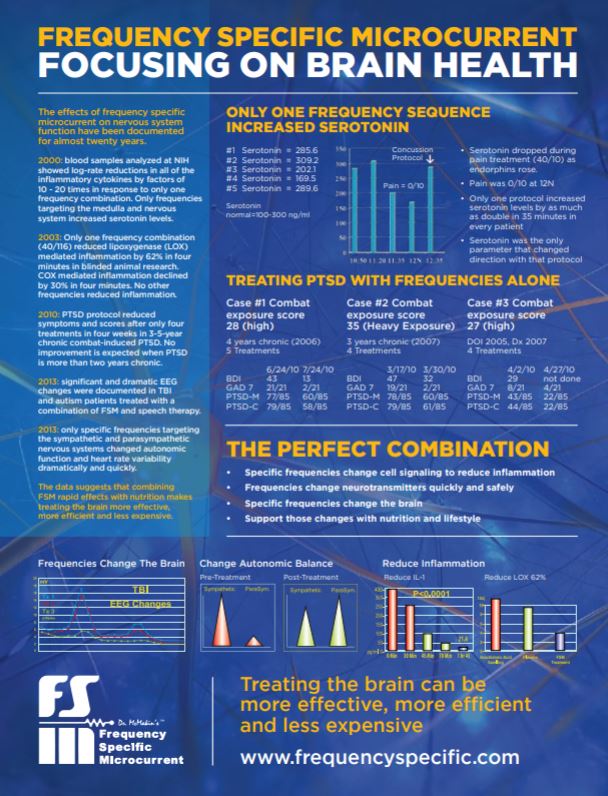
Carolyn McMakin, DC, makes the case that vagus nerve dysfunction plays a critical role in causing and perpetuating fibromyalgia. When we sustain an infection, injury, toxic exposure, or major stress, the vagus nerve maintains the integrity of our heart, lungs, digestive tract, immune and endocrine systems. Nevertheless, just like the brain, the vagus nerve will incur some level of dysfunction following trauma and chronic stress. McMakin proposes that treatment with microcurrent not only mitigates pain of fibromyalgia but also improves vagal nerve functioning.
Jacob Teitelbaum, MD, the author of our cover story, has devoted much of his medical career to understanding and treating fibromyalgia and chronic fatigue syndrome. Teitelbaum likens fibromyalgia treatment to playing a game of chess: “You can learn to play it in a few hours. And it takes a lifetime to master.” Of course, chess has a winner and a loser; hopefully, the physician and patient are both winners.
Unlike the high-tech aspect of some integrative clinics, Teitelbaum’s approach employs organized methodology readily available for practitioners and patients to use. He titles his treatment strategy, SHINE: Sleep and Sensitivities, Hormones and Hypotension, Infections, Nutritional Support, and Exercise. Teitelbaum has created a symptom questionnaire and treatment protocol available from him by emailing FatigueDoc@gmail.com. For the patient he has developed a questionnaire that sorts out the likely reasons for fatigue and pain and then delineates treatment recommendations from the SHINE Protocol: www.EnergyAnalysisProgram.com.
Teitelbaum is not unwilling to use pharmaceuticals in conjunction with nutrients, botanicals, and hormones. He has seen that patients respond to lower doses of multiple modalities, including drugs, rather than higher doses of fewer treatments. For sleep, his goal is eight hours of sleep and if that requires the use of drugs, then it requires the use of drugs. It is simply not acceptable to refuse prescribing drugs if all the natural remedies fail to achieve the refreshing level of sleep.
Of course, replacing and balancing hormones is critical for treatment of fibromyalgia. If the patient experiences orthostatic hypotension, increasing salt and water consumption, administering adrenal treatment, and compression stockings are recommended. Teitelbaum does treat infections but he does not make it his business to necessarily do numerous lab studies. Candidiasis diagnosis and treatment is determined by symptom history. Individuals with chronic sinusitis and/or irritable bowel syndrome require botanical and pharmaceutical treatment. He notes that patients with Lyme disease treated with antibiotics will require treatment for yeast. Patients who claim an allergy to an antibiotic should be reconsidered as having had a Herxheimer reaction rather than a true allergy.
Nutrient and nutraceutical support is essential for recovery. Teitelbaum offers recommendations of what has worked best with his patients. Special strategies are suggested for hypersensitivity and pain support. He reminds us mind/body/spirit approaches are also key to good health!
Jonathan Collin, MD
Publisher



