By Thierry Hertoghe, MD
Cortisol is essential for human life. To stay alive, humans need cortisol. Life is not possible without it. In the absence of cortisol, the sugar level drops below 30 mg/dl, and the systolic blood pressure drops below 50 mmHg, which will cause a patient to fall into a deep coma and die about 24 hours later(1-3).
Cortisol is also essential to enjoy a good quality of life(4-7). When the cortisol level drops below a threshold in the blood, life is experienced as increasingly more difficult and stressful. If the level of cortisol drops further, life literally becomes miserable and plagued with anxiety, fatigue, and suffering.
Frequency of Cortisol Deficiency in an Ambulatory Setting
How many individuals in a population are cortisol-deficient? Data about the frequency of cortisol deficiency is scarce, if nonexistent. One study reported that 7% of hospitalized patients received glucocorticoid therapy during their stay(8), but this percentage probably does not reflect the incidence of permanent states of cortisol deficiency in the global population.
An epidemiological study covering the whole population of Iceland over 18 years of age concluded that only 0.02% (22.1 per 100,000) of the population were suffering from primary adrenal deficiency(9). Spanish researchers found an even lower prevalence of 0.01% (10 cases per 100,000) in Spain suffering from Addison’s disease(10). These low numbers are based on the extremely low number of patients receiving the diagnosis of Addison’s disease and treatment for it in Iceland and Spain. Most cases are likely diagnosed with the traditional ACTH test, which is done with an inaccurate 250-fold too high dose (read further for more information). The numbers probably indicate that local physicians are not accustomed in diagnosing and treating primary adrenal insufficiency, leaving many cases of Addison’s disease undiagnosed.
To get more accurate information through broader investigations including both clinical and laboratory findings, together with my colleagues of the clinic, we investigated the prevalence of cortisol deficiency in 56 consecutive and untreated (not receiving any glucocorticoid treatment) patients visiting our clinic for hormone therapy for the first time (36 females, mean age: 50.6 years (20-78); 20 males, mean age: 42.3 years (20-61)). Depending on the severity of clinical and laboratory diagnostic criteria, 4%, 13%, 50%, or 84% of these patients can be considered cortisol-deficient and could potentially benefit from cortisol treatment(11).
Diagnosis was based on an association of both clinical findings and laboratory test results, and not on a single laboratory test or sets of signs and symptoms alone without a suggestive laboratory test.
The following five symptoms of cortisol deficiency were checked through a questionnaire filled in by the patient: low resistance to stress, fatigue in stressful situations, low blood pressure, sugar cravings, and allergic reactions (skin, ENT, and/or asthma). The five physical signs of cortisol deficiency that were assessed were hollow face, pigmented spots on the face, conjunctivitis, dark circles under the eyes, and wet palms (due to peak secretions of adrenaline and noradrenaline in stress situations compensating for the low cortisol levels). Thus, a list was made of five symptoms and five signs suggestive of cortisol deficiency. The simple presence of one of the complaints or signs, whatever its intensity, was considered as contributing to (but not establishing) the diagnosis of cortisol deficiency.![]()
The laboratory tests checking for diagnosis of cortisol deficiency included serum-free cortisol, 24-hour urinary-free cortisol, and 24-hour urinary 17-hydroxysteroids (i.e., the cortisol metabolites). We considered any test value below a critical level in laboratory tests as suggestive of (but not decisive for) the diagnosis of cortisol deficiency. The critical level was a level halfway between the average and the lower reference limit of the laboratory. The reason we used a critical level that is above the lower reference limit and not the lower limit itself is that the lower reference limit is a statistical – and not a health limit – and that many lower levels within the reference range are significantly associated with disease. These relationships are explained further in the paragraph on “Cortisol Reference Ranges.” For serum-free cortisol, the cutoff level was 12 (reference range: 7-27 ng/mL). For 24-hour urinary-free cortisol, the threshold was 30 (reference range: 10-90 µg/24 h). For the 17-hydroxycorticoids in 24-hour urines, the limit was fixed at 4.54 (reference range: 3.17-8.63 mg/24 h) in females and 7.5 (reference range: 6.10-11.70 g/24 h) in males.
Four categories of diagnostic criteria of increasing severity were applied to establish the prevalence. All of these criteria categories have medical legitimacy for diagnosis of cortisol deficiency.
The first type of diagnostic criteria is the presence of at least three of the ten possible signs or symptoms, with at least one of the three laboratory test results suggestive of cortisol deficiency. As shown in Figure 1, 84% of our patients fit into this category.
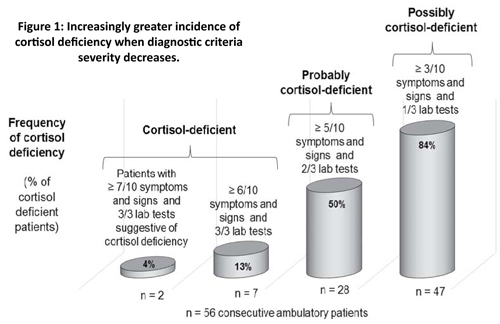
The second type necessitated the presence of at least five of the ten possible signs or symptoms, with at least two of the three laboratory test results suggestive of cortisol deficiency. As shown in Figure 1, half of the patients belonged to this category.
Criteria of the third category were severe. Only 13% of the patients presented the required minimum of six of the ten possible signs or symptoms and all three laboratory tests suggestive of cortisol deficiency, and could be classified in this group of undoubtedly cortisol-deficient patients. Only 4% (2 of 56) of patients belonged to the fourth group of severe diagnostic criteria with seven or more symptoms and signs and all three laboratory tests being conclusive.
The results of this small study show a high frequency of cortisol deficiency, which increases when criteria are less severe. They should not be considered representative of the general population but merely illustrative of the incidence of adrenal deficiency in a selected group within the general population, i.e., those individuals who are sent or go spontaneously to a clinic focusing on hormone therapy. The frequency of cortisol deficiency within this group is almost certainly greater than in the general population because many of our patients had levels in the lower third of the reference range in the laboratory tests(11).
Incidence of Cortisol Deficiency with Aging
Some studies have shown lower serum cortisol levels with aging(12-13), others no change(14), while several investigations showed higher levels, especially in the evening(15-16), which is at a time when the cortisol levels should considerably drop to allow the body to calm down and relax and prepare for sleep. However, as the metabolic clearance of cortisol decreases with age, thus allowing cortisol to remain for a longer time in the blood and less in the target cells(17-19), the higher evening cortisol level may not reflect a higher cortisol activity in the target cells.
On the contrary, cortisol metabolic activity may substantially decrease with age following a study that showed that the 24-hour urinary excretion of the 17-hydroxycorticoids – the main metabolites of cortisol (and, thus, a reflection of cortisol metabolic activity in target cells) – are nearly 80% lower: 2 mg/day in older adults compared to 9.3 mg in young adults!(20)
The Great Cortisol Discovery
In the mid-1930s, Kendall and Reichstein isolated several hormones of the adrenal glands, including compound E or cortisol, which was the most effective in prolonging the life of adrenalectomized animals. In 1946, Louis Sarettt succeeded in synthetizing cortisol for the first time. In 1948, sufficient quantities of compound E became available for the rheumatologist Philip Hench to test it successfully for the first time in a patient with rheumatoid arthritis(21-23). The improvement in this patient and others was so impressive that it triggered enthusiasm all over the medical world so that, in 1950, Kendall, Reichstein, and Hench soon after received the Nobel Prize in medicine for their work on cortisol.
However, three errors were and still are made with cortisol treatment, which have triggered controversies on cortisol’s use ever since and have probably made cortisol the most misunderstood and unjustly rejected treatment in medicine.
Three Therapy Errors That Spoil Outcome
What are these common errors? Firstly, excessive doses of cortisol were administered to quickly treat rheumatoid and other inflammatory disorders. Prolonged use of high cortisol doses reduces skin thickness, muscle volume, and bone density and provokes swelling, weight gain, bruising, pathological effects on the cardiovascular system, and at times a euphoric, excessively agitated character(8,24-27) in contrast, low doses of cortisol (i.e. 20-30 mg/day of hydrocortisone) or of one of its derivatives (5 mg of prednisolone for example) are relatively safe(28-31). In septic shock, a low dose appears to show efficacy in decreasing mortality, whereas a high dose does not(32-33).
Secondly, cortisol or its glucocorticoid derivatives were administered alone without the protection of other hormone supplements, such as DHEA (dehydroepiandrosterone – the other primary adrenal hormone), that prevents any excessive tissue catabolism from cortisol. In healthy individuals, each time the adrenal glands secrete the catabolic hormone cortisol, they also secrete protective anabolic hormones such as DHEA, androstenedione, and other androgens(19,34-39).

Thirdly, cortisol increases the supply of blood, oxygen, and nutrients to the brain, muscles, and inner organs by raising the blood pressure(53) through an increase in salt and water retention in the kidneys and vasoconstriction and through the stimulation of contractions of the thick smooth muscle layers that wrap up the arteries. Fourthly, cortisol “burns” fat(54-55). This lipolysis liberates energy.
A second important action of glucocorticoids is to reduce inflammation. Cortisol considerably reduces the migration of leukocytes into inflammatory zones(56-57). The accumulation of these white blood cells at the sites of inflammation causes swelling, compression, and pain. Cortisol also blocks collagen overproduction(57), which makes inflamed tissues thick and hard. Collagen is the main protein that fills up the spaces between cells in the tissues. By reducing collagen formation during inflammation, cortisol prevents fibrosis and, thus, formation of excessively thick scars or keloids and scleroderma, which is the disease that affects the skin and organs with fibrosis
At high doses, cortisol’s anti-inflammatory effect may atrophy the major immune gland, the thymus. However, thymus atrophy and immune depression only appear when cortisol treatment is imbalanced (i.e., too much cortisol without sufficient addition and protection by anabolic hormones and protein-rich foods). High doses of glucocorticoids without DHEA protection also produce skin, muscle, and bone atrophy, which are other well-known side effects of cortisol overdoses.
It is always the same story: too much of a good thing is too much. To use cortisol safely, it is important to administer physiological doses. In cases of higher needs, to the doses of cortisol can be temporarily increased if supplementary doses of anabolic hormones, such as DHEA, are also added.
By reducing inflammation, cortisol may also block the appearance of allergies. The increasingly higher frequency of allergies in people is partially due to pollution and intestinal problems – the known triggers of allergies – but is almost always a sign of adrenal deficiency. The adrenals glands do not secrete sufficient amounts of cortisol, which is the anti-allergy hormone. The loss of cortisol’s anti-inflammatory action also explains why cortisol-deficient patients typically suffer from intolerance to all kinds of medications.
Cortisol also provides beneficial effects through its insufficiently known antioxidant activity. Cortisol neutralizes free radicals preventing free radical tissue damage(58-60), a property especially useful in stressful conditions, which are associated with an increase in free radical production. Free radicals originate from oxygen molecules through the loss of an electron and become, for this reason, tissue-damaging compounds. The more free radicals are formed, the greater “oxidative stress” is inflicted on the body, thus damaging tissues, and the more tissues prematurely age.
Last, but not least, and contrary to belief, cortisol does not increase fat but breaks down fat(54-55). Weight gain that tends to appear with high-dosed cortisol supplements is not due to a direct stimulation of fat production by cortisol but through a stimulation of the appetite and an increased intake of weight-increasing foods, such as sugar and grains (bread, porridge, muesli, pasta, etc.).
Types of Cortisol Deficiency
There are three types of cortisol deficiency depending on the tissue that causes the deficiency. In primary cortisol deficiency, also called Addison’s disease (following the name of Dr. Addison, who was the first to describe the disease), the adrenal glands themselves are weak and unable to secrete a sufficient amount of cortisol. President Kennedy suffered from Addison’s disease and took a treatment for it(61). In secondary cortisol deficiency, the production by the pituitary gland of ACTH, the hormone that stimulates the adrenals to produce cortisol, is deficient. In tertiary cortisol deficiency, the production by the hypothalamus of CRH (corticotropin releasing hormone) that stimulates the secretion of ACTH is failing.
Diagnosis of Cortisol Deficiency
The diagnosis of cortisol deficiency is based on clinical and laboratory assessments confirmed by a successful therapeutic trial. To diagnose cortisol deficiency, laboratory tests (blood and urinary), an evaluation of all complaints, and physical signs of cortisol deficiency are needed. When sufficient findings suggest a cortisol deficiency, a glucocorticoid treatment trial should be engaged to confirm the deficiency. If the patient feels better, looks much better, and laboratory tests show no excess with the glucocorticoid therapy, then the diagnosis of cortisol deficiency is confirmed, and cortisol treatment should be continued. If the glucocorticoid treatment does not give any result, doses may be too low and a trial at higher doses should be undertaken. If the treatment provides overdose symptoms, even at low doses, then the treatment is contraindicated.
Donate today to contribute to our efforts!
Psychological Complaints of Cortisol Deficiency
Individuals with cortisol deficiency are tired(62-66) as soon as they have to exert effort or fall into stressful situations. People with adrenal deficiency lack the punch to react efficiently to stressful events. If they react, they quickly feel tired, even exhausted, and cannot face any new strains. If demands are high at their work, they end up being burned out, which is almost literally an “adrenal burnout” or a severe depletion of the adrenals stocks of cortisol-making patients no longer able to face normal daily life difficulties. Cortisol deficiency is the main deficiency behind the feelings of burnout.
The fatigue in cortisol deficiency has in my experience several characteristics. It consists of a lack of energy, flu-like feelings, a lower capacity to react well to stress, and a foggy feeling in the head. The lack of energy of cortisol deficiency(62-65) predominantly results from hypoglycemia – the lack of sugar. In stressful conditions, it exponentially worsens. The flu-like character of fatigue(67-68), where every part of the body feels uncomfortable, is due to the generalized inflammation of cortisol deficiency. The lack of punch to react to stress, typical of patients with cortisol deficiency, is due to low glycogen stores and low dopamine receptor numbers. The glucose stocks and dopamine activity are insufficient to increase the energy levels and cope with new stressful situations. Insevere cortisol deficiency, the lack of energy to react to events can become an inability to react, literally paralyzing the patient in stressful conditions where more energy is required. Coping with new stressors then becomes difficult or even impossible.
The fogginess and empty headedness of cortisol-deficient patients is due to a low blood pressure(69) that substantially reduces the blood supply to the highest parts of the body when standing, particularly the brain.
In the early stages of cortisol deficiency, patients may react very emotionally to events in an outburst of anger or anxiety, compensating for the lack of cortisol by peaks of adrenaline and noradrenaline. In later stages of increasingly greater adrenal deficiency, the adrenal medulla that secretes the catecholamines also wears out, leaving the patient without reaction to a new stressor. This severe situation is typical of burnout.
Cortisol-deficient patients are excessively sensitive to stress(70-73). They feel the world is stressful and difficult to live in because it is full of worries and aggressiveness. Cortisol-deficient patients tend to find that others, especially people close to them, family members, and colleagues at work, put excessive pressure on them.
Because of this feeling of excessive pressure, cortisol-deficient patients tend to be nervous and irritated. Irritability is the most typical psychological symptom of cortisol deficiency(74-76) due to increased secretions of adrenaline and noradrenaline. These neurotransmitters make individuals nervous and are secreted in higher amounts to compensate for the low cortisol. Outpourings of adrenaline and noradrenaline not only cause nervous behavior but also anger and anxiety outbursts.
In cortisol deficiency, the brain and nerves easily inflame. Brain inflammation makes patients feel that life is “inflamed,” more stressful, and even dramatic. This dramatization of problems and life events, which seems minor and easy to treat for healthy individuals, may appear to be extremely important and difficult to cortisol-deficient patients and make them use harsh, sharp words that reveal their inflamed perception of the world, such as “terrible,” “horrible,” “miserable,” “a catastrophe,” a disaster,” and “you are killing me.”
The Paranoid Behavior of Cortisol-Deficient Patients
Patients with cortisol deficiency suffer more than the average population would in similar stressful conditions. Because their suffering feels unbearable, they seek causes to their pain, hoping that they may find solutions by finding causes outside themselves. As it is easier to find a cause outside than inside of oneself, they tend to suspect others of being the cause of their suffering, often their closest relatives, such as the partner, family members, friends, or colleagues at work. In cortisol-deficient patients, a suspicion quickly becomes a conviction and transforms into accusations. They accuse others of being the cause of their suffering and tend to persecute them, surprising them by their overreactions.
The recurrent accusatory behavior explains the paranoid tendencies of cortisol-deficient patients and is the basis of the paranoid character typical to cortisol deficiency(76-79). One of cortisol’s roles is to reduce the production and levels of adrenaline and noradrenaline – neurotransmitters that make us overreact in a crazy, violent way and giving us the sudden desire to harm a person or oneself, sometimes even to murder or suicide!
The accusations form the base of the quarrelsomeness, which is another typical symptom of cortisol-deficiency. Patients tend to quickly interpret others’ offhand words as negative criticisms. In reaction, they utter sudden and violent accusations. In turn, these nervous reactions trigger heavy protest from the accused person in self-defense, and quarrels start over again. This quarrelsomeness induced by minor stresses makes life difficult for family members or colleagues at work.
Cortisol Deficiency and Stress
Cortisol deficiency complaints increase in intensity during stressful conditions. In calm, relaxing situations, patients with cortisol deficiency do not suffer much, if any, from their disorder. In stressful conditions, however, cortisol deficiency complaints come up and increase almost exponentially in intensity because these patients cannot make the supplementary amounts of cortisol necessary to cope with stress. Their adrenals barely make enough cortisol for the needs of an easy sedentary life where rest is central, and work or performance is secondary.
Healthy adrenal glands produce supplementary amounts of cortisol whenever supplementary work has to be done or whenever a dangerous situation occurs (i.e., to respond to the difficult situation, fight back, or run away from it). The energy comes from a higher sugar level, blood pressure, and number of dopamine receptors.
Inevitably, due to their negative life experiences, patients with cortisol deficiency tend to express negative thinking and have a low mood(80). Table 1, below, shows the most typical psychological complaints of cortisol deficiency.
Table 1. Psychological Complaints of Cortisol Deficiency
(Particularly frequent and intense in stressful conditions)
- Flu-like fatigue
- Outbursts of nervousness, anger, fear
- Lack of punch
- Use of intensely negative words: horrible, terrible, dramatic, disaster, the end of the world, etc.
- Poor resistance to stress
- Intense dislike of stress
- Irritability, aggressiveness, even meanness
- Try to avoid stressful situations, jobs, partner
- Quarrelsomeness
- Accusations, meanness toward others
Physical Complaints of Cortisol Deficiency
In adrenal deficiency, the body feels tense, particularly the muscles, due to high catecholamine levels, producing tachycardia and (heart) palpitations in stressful conditions. Wet armpits, wet hand palms, and wet foot soles occur in stressful conditions due to excessive sweating, also resulting from high adrenaline and noradrenaline secretions. The body tries to compensate for the lack of cortisol by increasing the secretion of catecholamines.
Other complaints are due to inflammation. Cortisol-deficient patients easily complain that the body hurts all over(81), including abdominal (digestive)(82-83), muscle(84-85), and joint pain(85-89), and even the hair and skin may feel unpleasant to the simple touch due to compression of the nerves by inflammation. Table 2 shows the physical complaints of cortisol deficiency. The same type of pain sensation is also seen during the flu. Patients with cortisol deficiency have a weak immune system that makes them prone to infections. They can get one infection after the other.
The flu puts people in a state of cortisol deficiency(67-68). The influenza virus blocks the secretion of ACTH, which is the pituitary gland hormone that stimulates the adrenal glands to make cortisol. The lack of ACTH causes the cortisol production to drop, and the flu-like symptoms of cortisol deficiency to appear(90).
A generalized lack of energy caused by low sugar levels is a predominant sign of the flu and of cortisol deficiency. A desire to lie down, caused by low blood pressure, pain aches in the whole body, and sore throat and red eyes initiated by inflammation are other dominant signs of the flu due to cortisol deficiency.
If cortisol supplements are taken in small bits (5 to 10 mg of hydrocortisone, for example) every half hour at the very beginning of the flu (in the minutes or first hour that the infection/inflammation begins), the flu disappears within one to two hours(91), as explained later when discussing cortisol therapy.
Table 2. Physical Complaints of Cortisol Deficiency
(Particularly frequent and intense in stressful conditions)
- Fatigue-like fatigue with the desire to lie down
- Deformed joints
- Tensed muscles
- Allergies: skin, nose-ear-throat with reddish coloration of inflamed zones, asthma, food allergies
- Tachycardia
- Intolerance to medications
- Palpitations, especially in stressful conditions
- Frequent infections: Sore throat, red eyes, ear pain, flu, etc.
- Excessive sweating in armpits, on hand palms, and on foot soles
- Reduced appetite
- Localized pains in structures that are put under pressure, such as the eyes, abdomen, joints, tendons, and muscles
- Weight loss in people caused by a low appetite
Physical signs of cortisol deficiency also predominate at physical examinations. Four types of signs are found differing from each other by their cause: hyperpigmentation, malnutrition, adrenaline excess, low blood pressure, or inflammation (See Table 3, below).
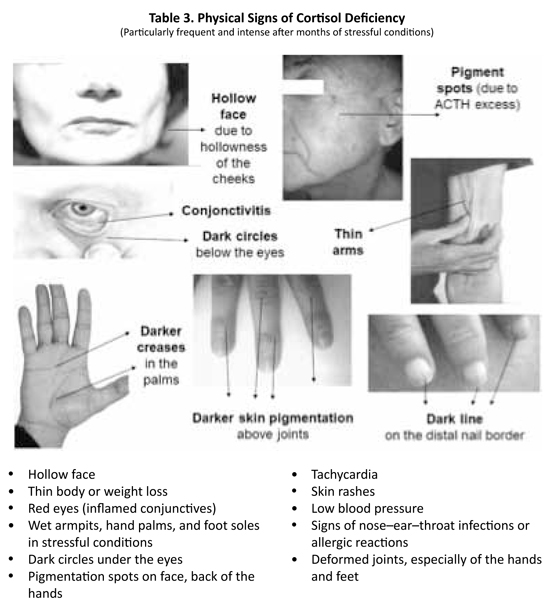
Pigmentation signs are specific to primary adrenal deficiency or Addison’s disease, where the adrenal glands are weak but not the pituitary gland, which overproduces the hormone ACTH to stimulate cortisol production(82-83,92-93). As ACTH is a pigmenting hormone, pigmentation increases with greater intensity in some areas: dark circles under the eyes, hyperpigmented skin folds, and spots on the face and body. In cortisol deficiency, the pigmentation is irregular and reflects desperate attempts by the body to increase cortisol production by the adrenals. When it is not successful, it pours down increasingly greater amounts of ACTH, pigmenting the skin, which darkens even without sun exposure.
Cortisol-deficient patients also tend to have a hollow face and often thin body(94-96) because they eat less or absorb the food less because their intestines are less effective at absorbing food.
The reduced food intake usually results from poor appetite, particularly for protein-rich foods, such as meat, because the nitrogen contained in the proteins tends to accumulate in the blood, a process called “azotemia.” The deficient food absorption in the intestines is the consequence of the inflammation of the intestinal mucosa, impairing its absorptive actions. Patients with cortisol deficiency also weigh less because they lack body water due to the loss of cortisol’s water-retaining effects.
As most patients overproduce adrenaline and noradrenaline to compensate for the cortisol deficit, signs of adrenaline excess, such as wet armpits, palms, and soles and trembling fingers, tachycardia (95), and acute systolic hypertension (the “white coat” arterial hypertension) may be found during the physical examination.
As cortisol is also a hormone that raises the blood pressure, the blood pressure is often low at rest in people with a lack of cortisol(69,97-98). Finally, signs of inflammation are often found due to the loss of cortisol’s anti-inflammatory effects: conjunctivitis, otitis, rhinitis, eczema(99-100), psoriasis, arthritis (with joint deformations, especially in the fingers)(101-105), gastritis, enteritis, colitis, and so on.
Cortisol deficiency favors the development of the following pathological conditions: allergies, including asthma and eczema, and generalized inflammatory diseases, such as rheumatoid arthritis(101-105), lupus erythematosus disseminatosus(106), systemic sclerosis, etc. Also, Hodgkin’s disease and lymphomas may be facilitated by cortisol deficiency, as these diseases tend to regress with cortisol treatment(107-109).
Laboratory Tests to Screen for Cortisol Deficiency
Three types of cortisol tests may help diagnose cortisol deficiency: blood, saliva, and 24-hour urine. They are all complementary to each other.
Firstly, blood or, better, serum tests of total cortisol(110), free cortisol, and transcortin (the protein that transports cortisol to the target cells in blood)(111) can be assessed. Total cortisol consists of all cortisol found in the blood, regardless of whether it is bound or not to a transporting protein. Free cortisol is the small fraction of total cortisol that is not bound to any protein and easily diffuses into cells. The usefulness of testing for transcortin is that high levels of this transporter attach to cortisol excessively, so it remains in blood much longer, not sufficiently getting into the target cells.
In the previous study where the prevalence of cortisol deficiency in our clinic was studied, we also checked the relationship between clinical findings and serum levels of free cortisol in 55 consecutive patients (36 females, mean age: 50.6 years; 19 males, mean age: 42.0 years). The study showed that serum levels of free cortisol reflect the number of signs and symptoms of cortisol deficiency relatively well through an inverse association. Progressively lower serum-free cortisol levels are observed with increasingly greater numbers of clinical signs and symptoms (on a scale from 0 to 10) as pictured in Figure 2, below(112).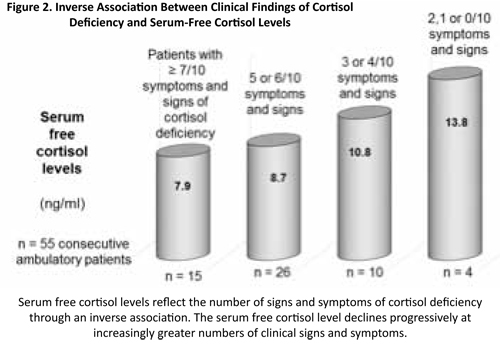
The ACTH-stimulation test is another blood test that evaluates the adrenal reserve, whether the adrenal glands have sufficient cortisol stored to supply supplementary cortisol in case of increased need. Injecting ACTH, the pituitary hormone that stimulates the secretion of cortisol, into a vein directly stimulates the adrenal glands. Check it every 30 minutes by withdrawing a blood sample and measuring the increase of cortisol obtained. Any doubling or more of the level of cortisol from the initial level indicates an adequate adrenal reserve and the likelihood that there is no cortisol deficiency. Unfortunately, in most clinics, the test is done by injecting 250 µg of ACTH, a huge overdose. Almost any adrenal glands, even weaker ones, will react to this overdose. Two studies have shown that using a more natural or physiological dose of 1 µg of ACTH allows for a much better differentiation between patients with adrenal deficiency from subjects without it. Whenever the cortisol level does not double with ACTH (whatever the initial serum cortisol level is), it indicates an intermediate degree of deficiency in the adrenal reserve(113). Studies have shown that critically ill patients in emergency rooms whose adrenal glands do not secrete enough cortisol after an ACTH injection die in the following days and weeks, while most other patients with good ACTH test survive(114-115). Thus, an abnormally low ACTH test helps detect critical persons who need a cortisol supplement for survival.
The saliva cortisol test checks the cortisol circadian rhythm with four samples taken at distant times(116-117). A higher morning peak of cortisol must appear in this test. Burnout patients usually have an insufficient morning cortisol peak. In the most severe cases, the cortisol morning rise may even be absent, and the cortisol circadian rhythm flat and inexistent.
The 24-hour urine test evaluates the excretion of cortisol and its metabolites in the urine during a full day and night cycle. The urinary cortisol level in this test reflects cortisol production during a 24-hour period(118-124). The measurement of cortisol’s major metabolites, the 17-hydroxycorticoids, informs on cortisol’s metabolic activity – how much cortisol is really used for action – during the same period(125-128). It is important to collect baseline urinary excretions of adrenal hormones, which are representative of the patient’s adrenal activity, not stress-induced ones. Patients should therefore collect their urine in relaxed, sedentary conditions during the 24 hours that precede the test and during the 24 hours of the urine collection) to avoid increases in cortisol metabolites due to physical activity or high-stress conditions.
In all these tests, the measurements of protective anabolic hormones, such as DHEA, the sex hormones, and IGF-1, should be included, as most treatments with cortisol include one or more of these hormones in the treatment to ensure an adequate catabolic/anabolic hormone balance.
Cortisol Reference Ranges
Cortisol reference ranges are statistical ranges, not health ranges. If the reference range for cortisol in laboratory tests would be a range of serum levels corresponding to health, cortisol deficiency would only be diagnosed in 2.5% of the population, those whose cortisol level is below the lower reference limit.
However, the laboratory reference limits for cortisol are purely statistical parameters. Just as for other hormones, 2.5% of the population statistically have a cortisol level above the upper limit, 2.5% have a value below the lower limit, and the cortisol level of the remaining 95% is within the reference range(129), regardless of whether these subjects have a deficiency. The laboratory “normal” limits are, thus, not limits separating “healthy” levels, which would be all the levels within the reference interval, from the levels that are below or above the reference interval and that would correspond to levels of cortisol deficiency or excess. Reference limits only indicate where a patient’s hormone level is compared to that of other patients who attend that laboratory.
Even if an entire population is deficient in a hormone, such as postmenopausal women who are all deficient in estradiol, 95% of this population would still have a hormone level within the reference range.
Both low and high serum cortisol levels within the reference range are associated with increased risks of pathology and mortality. Hormone levels are not necessarily adequate when they are within the “normal” range between the upper and lower reference limits of the laboratory tests. On the contrary, for most hormones – including cortisol – scientific research has shown that many serum levels within the reference range are significantly associated with disease and even mortality(130-150).
Researchers have shown that serum cortisol levels within the reference range but near the lower reference limit are usually inadequate because they are associated with an increased likelihood of disease, suggesting that these lower levels within the reference range should also be treated. In my experience, borderline low limits are also associated with complaints and physical signs of cortisol deficiency. Studies have also shown that cortisol levels near the upper limits may be associated with an increased risk of disease, suggesting that the optimal cortisol level in sedentary conditions should be an average level, neither too high nor too low. However, in stressful situations, cortisol levels may need to increase to provide additional energy to respond to the stress; this is the reason that levels near the upper limit were associated with better outcome than lower levels in some studies.
Table 4
Table 4 shows an overview of several of the studies showing the association of serum total cortisol levels within the reference range with increased risk of psychological and physical disease, and premature death.
Cortisol Binding Globulin (Transcortin)
High serum levels of cortisol binding globulin (CBG or transcortin) often cause intracellular cortisol deficiency. For a correct evaluation, physicians should also check the serum level of cortisol binding globulin, the main plasma protein that binds cortisol and transports it to the target tissues. The ideal transcortin level in the plasma is situated at the average or slightly below the average of the reference range. High concentrations (positioned in the upper half of the reference range) to very high levels (above the upper limit) of CBG are usually excessive because they bind excessive amounts of cortisol, literally “imprisoning” cortisol in the blood(151). This cortisol sequestration in the blood prevents most of it from penetrating into target cells and exerting their beneficial effects, thus producing – at least a mild degree of – intracellular cortisol deficiency.
A good example of excessive CBG levels with intracellular and, thus, physical and mental cortisol deficiency can be found in women who take birth control pills(152-153). The estrogen compound of these pills makes the women’s livers overproduce transcortin through the accumulation of the pill’s estrogen compound in the liver after absorption.
Cortisol Deficiency: Part 2 addresses treatment options for cortisol deficiency
Born in Antwerp, Belgium, Dr. Hertoghe practices his medicine in his clinic in Brussels. With his sister, Dr. Thérèse Hertoghe, they proudly represent the fourth successive generation of physicians working with hormonal treatments – and this since 1892 (after Eugène Hertoghe, former vice president of the Royal Academy of Medicine in Belgium, and Luc and Jacques Hertoghe, endocrinologists). Dr. Thierry Hertoghe devotes his life to the promotion of a better, patient-oriented, and evidence-based medicine.
Author of numerous books, Dr. Thierry Hertoghe also travels a lot to take part in numerous conferences and congresses throughout the world. He co-organizes many of these specialized gatherings and holds important positions in several international and national medical organizations (which usually tend to fight against aging). He is the president of the International Hormone Society (over 2500 physicians), and of the World Society of Anti-Aging Medicine (over 7000 physicians), as well as the supervisor of two important postacademic trainings for doctors.
Click here for the full list of REFERENCES from both Part One and Part Two.



